Evaluation of the public health clinical rotation in medical school: a qualitative case study design
Article information

Abstract
Public health clinical rotation in the Faculty of Medicine, Universitas Islam Indonesia, was conducted in Puskesmas (community health center). This study aims to evaluate the public health clinical rotation in Puskesmas, part of the clinical clerkship of the Faculty of Medicine, Universitas Islam Indonesia. Several concerns have been highlighted regarding the implementation of clinical rotations in public health in Puskesmas. A briefing session before placement in the village must be coherent with a guidebook. The placement of students in the village was based on community health issues determined by the Puskesmas supervisor. Priority in the curriculum was given to converting the alertness village (Desa Siaga) into a Program Indonesia Sehat-Pendekatan Keluarga (Healthy Indonesia Program-Family Education) program throughout implementation. Moreover, scheduling after four major clinical programs was difficult, and the writing of reports served as a guide for establishing the correct format. Therefore, the objective of the evaluation was to assess knowledge, skill, and psychomotor, and the burden of assignment in Puskesmas was difficult to accomplish a primary task in the community.
Introduction
The Indonesian Medical Council (Konsil Kedokteran Indonesia, KKI) established a curriculum for medical education that is typically divided into two phases: preclinical and clinical [1]. The duration of the preclinical phase is 4 years, followed by the clinical phase duration of 2 years. Moreover, early clinical exposure and community-oriented programs in the public health curriculum are undertaken in Puskesmas [1]. Puskesmas is a government-managed public primary health facility that provides individual or community health services in designated locations [2]. Multidisciplinary teamwork and comprehensive programs Puskesmas in individual and community, including health promotion, surveillance of communicable diseases, family planning, and environmental hygiene, are appropriate for medical students in public health clinical rotations involved in those programs [3]. Nevertheless, public health courses are frequently utilized to fulfill a variety of objectives in a number of public health-related themes, including health economics, biostatistics, epidemiology, child and maternal health, and mortality and morbidity calculations [4,5]. These courses must be further integrated with various medical curriculum types that cover preclinical and clinical phases, such as anatomy, physiology, and clinical diseases [4]. This condition shows the difficulties educators face when addressing public health issues with the population and community. There is a gap and disconnection between topics and clear objectives are required. Hence, these concerns exacerbate the confusion among medical students regarding public health subjects [5].
Every Faculty of Medicine is required to apply the curriculum in a clinical rotation, which includes public health. In the Faculty of Medicine, Universitas Islam Indonesia (FM UII), the 8-week public health curriculum consists of six core modules, namely, management of intervention, epidemiology, health promotion, health and safety at work (HSW), health finance, and elective. The learning process in every module consists of guidance, supervision, oral exam, written exam, case reflection, and journal reading. Students are placed in a village supervised by a supervisor from Puskesmas. Each year, the clinical phase rotation in public health is assessed, but the evaluation must provide insight into a curriculum suitable for students. Meanwhile, the Ministry of Health (MoH) has already developed several regulations regarding health services, including the implementation of the National Health Insurance and Gerakan Masyarakat Sehat (GERMAS) program or healthy community movement [6]. Consequently, every medical faculty should modify the public health curriculum in light of the present policy in health services. Hence, this study assesses the public health curriculum during the clinical phase in FM UII from the perspectives of students and educators to offer insight into suitable programs.
Methods
1. Study design
A case study design is a research method that facilitates the examination of phenomena within a given context by employing various types of data sources [7]. In this manner, the issues are not revealed through a single aspect but rather through multiple ones that allow diverse perspectives to be articulated and comprehended from various sources, including contextual information [8]. A case study ensures that an intriguing topic is thoroughly described and that the points of a phenomenon are presented, but the methods are distinct and deserving of discussion [9]. In this study, the evaluation of the well-revealed public health clinical rotation program in FM UII was the focus. However, the methods of delivering the public health curriculum were different among faculties of medicine. This study was conducted in two affiliated Puskesmas in Magelang and Sragen regencies in 2018. Due to the established memorandum of agreement to implement public health clinical rotation in FM UII, these two regencies were selected.
2. Theory of evaluation system in education
We based our evaluation system theory in medical education on a thesis by Wilkes and Bligh [10] in 1999 called the evaluation cycle. This model consists of four domains of the system, namely, teaching and learning activity, collection and assessment of evaluation data, reflection and analysis, and planning and preparation. Fig. 1 shows the evaluation cycle.
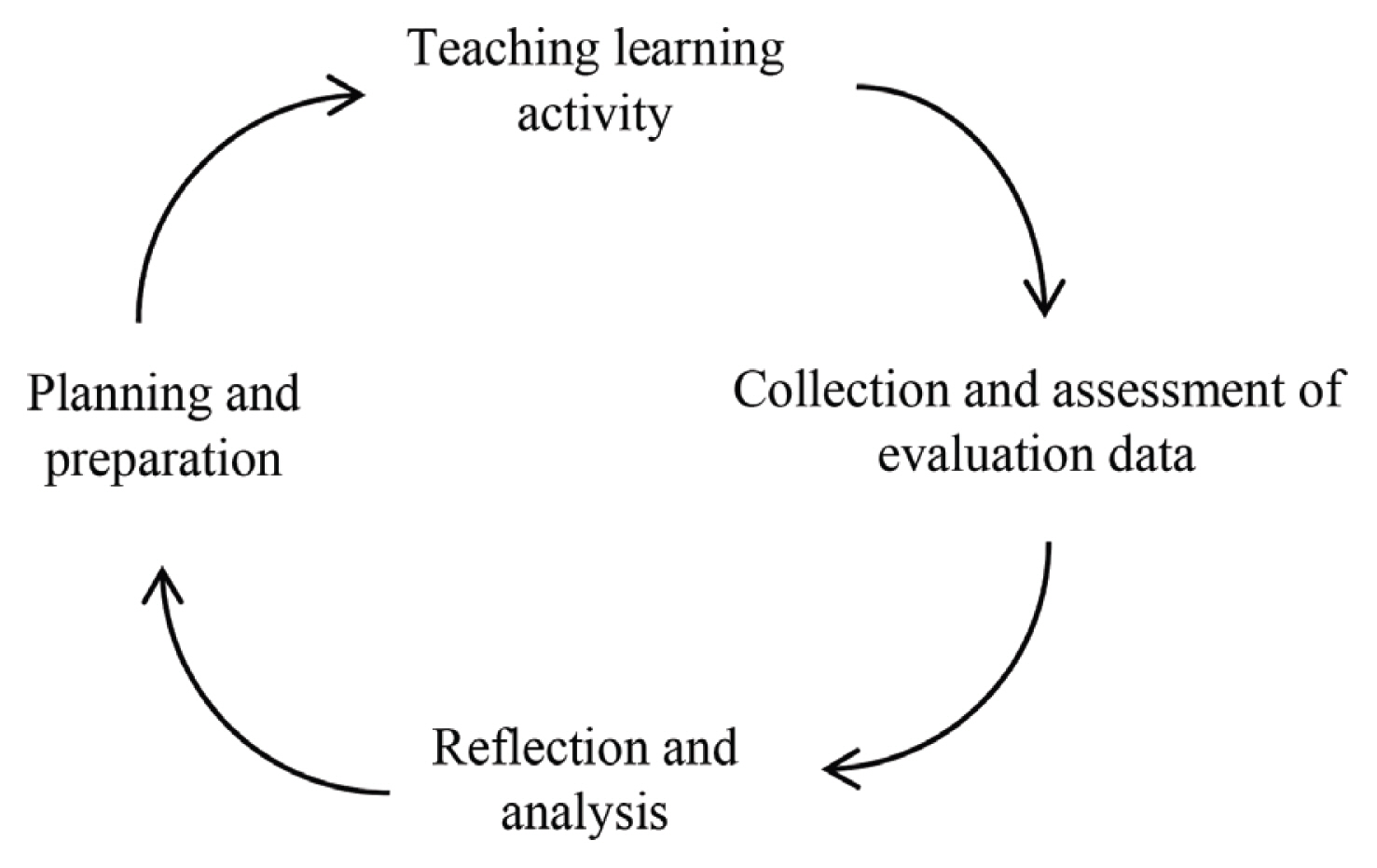
Evaluation Cycle in Medical Education
As shown in Fig. 1, our study started with teaching and learning activities in public health clinical rotation. We addressed six modules of clinical rotation: management of intervention, epidemiology, health promotion, HSW, health finance, and elective. The objective was to provide students’ and supervisors’ reflections on their experience during 8 weeks of rotation to complete those modules in combination with additional assignments in Puskesmas. The Program Indonesia Sehat-Pendekatan Keluarga (PIS-PK; Healthy Indonesia Program-Family Education) program has been integrated into the module of management intervention. The subsequent session collected and assessed data based on interviews and discussions with students and supervisors. This step aims to get an answer, challenge, and opportunity during the learning process in Puskesmas. Additionally, we conducted a reflection and data analysis to obtain accurate information and combine it with the law and national regulations in medical education. Finally, planning and preparation for corrective action for the other curriculum were adopted based on the result of this study.
3. Public health clinical rotation pathway
As shown in Fig. 2, the clinical rotation in the public health course in FM UII consists of three pathways: preparation, implementation, and evaluation.
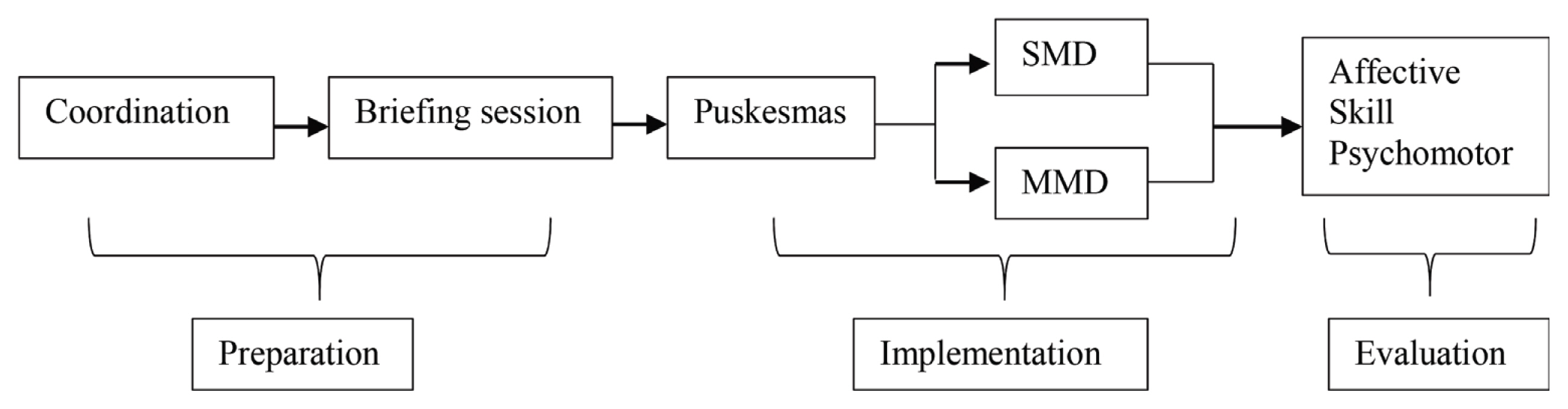
Public Health Clinical Rotation Scheme in the Faculty of Medicine, Universitas Islam Indonesia
SMD: Survey Mawas Diri, MMD: Musyawarah Masyarakat Desa.
4. Data collection
A judgmental sampling technique was proposed to collect respondents. In this technique, information was gathered according to the examiner’ judgment, expertise, or knowledge of the respondents’ target in implementing clinical rotation in public health. In this study, three supervisors in the Public Health Department of FM UII, three supervisors in Puskesmas, five students from Puskesmas in Sragen regency, and five from Puskesmas in Magelang regency were involved as respondents. Thus, there were a total of 16 respondents. Six sample supervisors were suitable respondents in this study because they were relatively homogenous. The selected supervisors had at least 1 year of experience supervising clinical rotations for students. To collect information from the supervisors at the Public Health Department and Puskesmas, an in-depth interview was conducted using a semistructured questionnaire and was guided interactively. Meanwhile, to collect information from the students who accomplished public health rotations in Puskesmas, a focused group discussion (FGD) was carried out. In FGD, a research assistant led the process with a provocative question. During the clinical rotation, the students expressed their experience without interruption until the data in every question were saturated. One research assistant led the FGD with a semistructured questionnaire. Both data collection methods were conducted until saturation, in which new data did not inform new perspectives regarding the topic [11].
5. Analysis
Both in-depth interviews and FGD were recorded, transcribed verbatim, anonymized, and then analyzed via content analysis. Two authors (S.R.S. and P.L.G.) read and analyzed the transcript for the topics arising during the open coding process. Informed consent was obtained from all individual participants included in the study. Finally, the ethics proposal was submitted to FM UII with protocol number 10/C/IX/19.
Results
Table 1 identifies three major themes, subthemes, and core findings. The themes include clinical rotation preparation, implementation, and evaluation.

The Difference between Video-Based and Classroom Teaching Based on Students’ Evaluation and Educational Level
1. Theme 1: preparation
In this category, we extracted two categories: placement in Puskesmas and village and briefing session, as presented in Table 1. In selecting the village around Puskesmas, the supervisor should determine which villages have community health problems:
“I choose a village with a priority of health issues. A few moments ago, I chose a village with many mental problems among the residents. We also need assistance to establish a ‘mentally healthy village’ program, so I decided to place students in that village. At least, they can make a structure and organization of ‘mentally healthy village’ because the human resources in Puskesmas are limited.”
This study found that students complained about the briefing session. The students perceived different explanations between the briefing session and the guidebook, making them confused:
“The explanation in the briefing session is different from the guidebooks. For example, previously, it should be about HSW topic, but technically the Health and Safety Executive (HSE) module was not explained in the briefing session. So, we sometimes missed the information about the technical HSE program in the guidebooks.”
A supervisor added that briefing sessions with a guidebook are complementary:
“It is intentionally different. It does not make sense if it is similar between the guidebooks and the class. Students can read the guidebooks for detailed programs, but a comprehensive explanation in every module can only be obtained in class. So, the material in class is supplementary for the guidebooks.”
2. Theme 2: implementation
In this theme, we extracted three subthemes: curriculum, scheduling, and writing report, as presented in Table 1. The students performed a survey called “Survey Mawas Diri” (SMD) and a conference named “Musyawarah Masyarakat Desa” (MMD) to obtain priority health problems in the village:
“The first week is orientation and following every occasion in Puskesmas, then data observation in Puskesmas. In my case, I asked students to go to the village with me, communicate with community figures, and take preliminary data there. So, they can join and engage with community programs directly in the village.” “Therefore, we asked students to learn SMD and MMD. Even though in Puskesmas, we have numerous secondary data, we encourage them to get the data directly in the village. They will analyze the data and prioritize which one will be given intervention based on their analysis.”
The supervisors in two Puskesmas encouraged to propose the PIS-PK program as a new curriculum:
“At first, clinical rotation in public health was community-oriented, focusing the program in the community or village based on ‘Desa Siaga’ program. Solving the problems using PHBS indicators and instruments to analyze community-oriented problems. However, since the new regulation of PIS-PK, identification of problems has changed from community to family-based.”
“PIS-PK program has the intention to collect the data in accordance of healthy community movement (GERMAS), in the PIS-PK, all of the family health data belong to Puskesmas, and then intervention with a family approach in the context of GERMANS program.”
FM UII used “Desa Siaga” or the Alert Village program as the guidelines for the current curriculum. The curriculum elaborated significant aspects of community rather than family-focused aspects:
“So, according to the report I read, the family approach in family medicine is superficial. Students tend to elaborate on the community aspects more than family-focused aspects.”
The students must be able to diagnose and make prescriptions in Puskesmas. They were assisted in Puskesmas to handle the patients:
“In my opinion, the public health curriculum is the implementation of science and skills that we have done before. We have just done two clinical rotation programs, and a group of students accomplished only one program. It was too early for us to conduct the public health rotation. If we have done all of the clinical rotations in the hospital, we can understand diseases and apply it in the public health curriculum.”
Consequently, students who had yet to accomplish the four major programs gave incorrect prescriptions to patients:
“It happened previously. I asked students to assist in the children’s ward, but a midwife complained about their prescriptions. Also, a pharmacist said that a student gave a prescription to children as if they were adult patients, and then she returned the prescription to me. Eventually, I am afraid to give the prerogative to students to write prescriptions.”
FM UII had modified the clinical rotation to accommodate students’ preferences, but placing public health rotations after those major clinical rotations were formidable:
“That is our problem. It is difficult to locate public health after four major programs, ideally after four majors, but in fact, the implementation is difficult.”
The problem in writing the reports was the need for an ideal format that the students expected to be established:
“Actually, there are lists to make a report in the guidebooks. Usually, we are more familiar with writing it from examples. However, the reports are also different for every student. If possible, an ideal format and example of a report are established, and we just fill out the form directly.”
3. Theme 3: evaluation
In this theme, we extracted two subthemes, competence in a clinical rotation in public health course and assignments, as shown in Table 1. The evaluation consists of three major domains: affective, skill, and psychomotor. Therefore, supervisors in the department and Puskesmas gave assessments based on student performance:
“We tried to assess student’s affective performance based on attitude and behavior called condite assessment. Psychomotor can be measured students’ skill in handling patients in Puskesmas and community engagement and knowledge based on an examination, oral or paper-based examination.”
The burden of assignments in Puskesmas faced difficulty of students to accomplish programs in community:
“Puskesmas must be given an explanation by FM UII about the position of students, whether in health services or community. We were confused in between both. On the one hand, Puskesmas asked us to assist in the policlinic, emergency room, or pharmacy. On the other hand, we have a mandatory assignment in the community···”
Discussion
Public health clinical rotation commenced with a briefing session. Before the placement in the village, the students are briefed about the concept during clinical rotation. Our study revealed that the briefing session required a guidebook to be more precise. The contents varied between class and a guidebook. The difference in the content is because the briefing session detailed what students do in Puskesmas and village. However, a guidebook is superficial guidance in conducting an activity. A guidebook consists of rules, an assessment form, an outline of the module, and a signature. Since the public health clinical rotation is different from the hospital-based rotation, the briefing provides superficial insight into the curriculum. The educator must assist students in the transition period to reach the goal in the clinical rotation. A briefing session is more than superficial information but stimulates learning objectives. The intended information provides an understanding of the component that students will encounter at the study site [12].
The decision on the village of health intervention becomes the privilege of Puskesmas. The eligibility criterion for selecting Puskesmas is the availability of a supervisor. The supervisor is a medical doctor in charge who has been trained to perform and understand the detailed contents of the curriculum. Our study obtained that Puskesmas enable capturing the most suitable village to perform community health intervention. There is no specific criterion of the village to consider. Since both Magelang and Sragen regencies have the characteristic of distribution and determinant of disease almost similarly [13].
During implementation, students performed SMD and MMD, a component of Alert Village. The curriculum scope in FM UII is focused on Alert Village because the policy encouraged the community to be the leading sector in primary health services relevant to the core curriculum in public health [14]. Thus, public health clinical rotation aims to encourage students to be part of the community to run and make the Alert Village program succeed in both Sragen and Magelang regencies. However, the alertness of the village must be more rational with the current policy. A further method should apply to the PIS-PK-based policy.
Since the first week of clinical rotation, the students have been encouraged in the community to build engagement during SMD and MMD. Both components were community-based empowerment in the Village Alert program. This program aims to screen health problems in the community, identify causal factors of health problems, and map community resources to solve those problems [6]. Findings from the SMD should be brought to MMD to map and list the priority of the health problems. The public health curriculum stands in this survey to engage with the community. The SMD and MMD are important components of the community-based Alert Village programs. Changing from a community-based to a family-based strategy is vital for public health education.
The MoH has mandated a new paradigm for health services termed PIS-PK, which emphasizes a family-centered approach. The family-based approach is a development from the home visit program by Puskesmas and an expansion of its community health services, which include home visits and family profile collection, data updates, health promotion and prevention, and follow-up programs after health check status in Puskesmas [15]. Components of family doctors include person-centered care, community-oriented activities, particular problem-solving skills, a comprehensive approach, and holistic primary care management modeling [16,17]. Our study stated that students required a novel health service paradigm, switching from a community-based to family-focused agenda. Noteworthily, the World Organization of National Colleges, Academic and Academic Association of General Practitioner/Family Medicine (WONCA) modifies the PIS-PK program.
Additionally, scheduling for public health clinical rotation was difficult. This study determined the preferences of students to accomplish internal medicine, obstetrics and gynecology, pediatrics, and surgery modules before public health rotation in Puskesmas. However, this would completely disrupt the scheduling for clinical rotations. The placement in the public health program at the end would accrue students, but the ratio of students to supervisors would be high and burden supervisors, resulting in inefficient supervision. The scheduling in clinical rotation based on the KKI regulation elucidates clinical rotation for students to be 2 years. Every Faculty of Medicine has the authority to adjust or modify the curriculum content at 20% [1]. In this case, adjustment of clinical rotation for public health following hospital clinical rotation is difficult, as it may result in problems, such as incorrect prescriptions. Howard et al. [18] reported that clinical rotation schedules must balance individual preferences, compliance with the rule, and institutional staffing requirements. Effective scheduling will enhance students’ satisfaction.
Meanwhile, writing a report is a component of assessment in clinical rotation. A report worthy of writing should encourage students to achieve multiple educational values and reflect on their studies; however, good mentorship and training are also necessary [19,20]. Our result, however, indicated that there was no example of a preferred report format among the students. FM UII has determined the format list in a guidebook that must be followed by students. Additionally, there was no example of a report in every module. This finding raised our concern about writing an example of a report.
Both supervisors assess the evaluation of clinical rotation. This evaluation aims to verify that public health modules are applicable and that students retain knowledge to pass the exit exam to become medical doctors [21]. Evaluation is used for corrective action and continuous improvement in public health studies. Additionally, the students complained about additional tasks in Puskesmas. Due to the burden of assistance in Puskesmas, they experienced difficulty accomplishing their assignments. Assignments during clinical rotation in Puskesmas were focusing on patients-centered approaches. This method improves skill, knowledge and experience to the real case in community and collaborations to other health-care workers [22]. Students can learn directly from the real patients, exploring their symptoms and finding the signs of a disease. In this manner, FM UII did not communicate to balancing the assignments in Puskesmas with community tasks in SMD and MMD programs. A robust communication between FM UII and Puskesmas is important to tackle this issue.
Our study had several limitations. First, this study was conducted in a single institution, FM UII. As a private organization, we implement the public health curricula differently, exclusively with a state-based university. To mitigate this constraint, we piloted an informal discussion with the neighboring university to catch the perspective implementation of the curriculum. Second, guideline implementation of public health curriculum by medical education collegium is insufficient to cover community problems. Few of the contents are based on clinical issues related to community problems. To diminish this issue, we only take the most common contents in the guideline that is implemented in our institution. Third, selection bias results from supervisors in Pukesmas lacking knowledge about the curriculum. To lessen this problem, we selected more experienced and trained supervisors who have been supervising since the start of the clinical rotation.
Further investigation is necessary to evaluate the public health clinical rotation program by involving multicenter universities and the best practicing public health curriculum to ensure that this educational pathway succeeds in enhancing students learning outcomes in the public health clinical rotation.
In Indonesia, public health clinical rotation is an obligation for medical students prior to being certified as a physician. Nevertheless, the regulation of MoH in health services has replaced the Alert Village with the PIS-PK. Consequently, based on the current policy that focuses on the role of family doctors in the community, FM UII modifies the curriculum. FM UII draw attention to several findings, including briefing sessions are coherent with guidebook, placement students in village, writing report format, scheduling after four major clinical programs, and evaluation in examination and burden of assignments.
Acknowledgements
We thank to medical students, supervisors in faculty of medicine and Puskesmas who participated in this study. We also thank to Heni Ari Nur Rohmawati from Vernacular Edu for proofreading this manuscript.
Notes
Conflicts of interest: Sani Rachman Soleman receives fellowship grant from the Japan Society Promotion Science (JSPS) for his doctoral degree. Except for that, no potential conflict of interest relevant to this article was reported.
Author contributions: PLH planned, surveyed, and collected the data. SRS collected and analyzed the data. Both authors wrote and reviewed the manuscript.
Funding: This study was funded by Faculty of Medicine, Universitas Islam Indonesia with program “Hibah Penelitian Kolaborasi”.