Factors predicting rural location employment intent and choice among medical students and graduates
Article information

Abstract
Purpose
Workforce shortage is a contributing cause of health inequality in rural Australia. There is inconclusive evidence demonstrating which factors cause doctors to choose rural practice. This study’s objective is to determine predictive factors for medical students’ intent to work rurally and for graduates’ current rural employment location choice.
Methods
This prospective cohort study, utilized data gathered from the University of New South Wales about students and graduates who had spent one or more years in a Rural Clinical School. Participants were final year students and graduates already working in Australia. Stepwise logistic regression was used to determine predictive factors for the two outcomes.
Results
Predictors for student intent to work rurally are rural background (odds ratio [OR], 7.16; 95% confidence interval [CI], 2.59–19.53), choosing to study at the Rural Clinical School (OR, 8.72; 95% CI, 1.32–57.63), and perceiving rural areas as opportunistic for career advancement (OR, 1.69; 95% CI, 1.15–2.49). Predictors for graduates currently working in a rural location are Bonded Medical Program participation (OR, 6.40; 95% CI, 1.15–35.59) and personal altruism (OR, 1.91; 95% CI, 1.02–3.57).
Conclusion
While intent is predicted by having a rural background, choosing to study at the Rural Clinical School and perception of rural areas as having positive career opportunities, a current rural workplace location among graduates is predicted by holding a bonded medical position and a desire to serve an under-resourced population. Maintaining the Bonded Medical Program and clear communication regarding training pathways may increase numbers of rural doctors.
Introduction
1. Background/rationale
Medical workforce shortage among rural and remote communities significantly affects the Australian population as well as approximately 50% of the global population who live outside urban centers but where only 25% of the global medical workforce practice [1].
Classification of rurality for university admission and return of service obligations in Australia is defined by the Australian Statistical Geography Standard–Remoteness Area (ASGS-RA) [2]. Twenty-eight percent of Australians live outside major cities and they experience health inequality (e.g., 1.4 higher morbidity rate) correlated to remoteness area. Workforce shortage has long been recognized as an issue contributing to rural health inequality. In 2000, the Rural Clinical Schools (RCS) Program was launched by the Australian Federal Government, aiming to increase numbers of rural (ASGS-RA 2–5) medical students and mandate rural exposure for all medical students. By 2011, 23.6% of domestic university students were from rural backgrounds [2].
Other governmental schemes incentivize rural practice for individuals (e.g., the Bonded Medical Places [BMP] scheme, launched in 2001 and companion Medical Rural Bonded Scholarship [MRBS]) by providing conditional financial assistance during medical school in return for practice in ASGS-RA 2–5 locations during their early post-graduate career. The trajectory of the BMP has been criticized for the lack of post-graduate training opportunities in regional locations, for specializations other than general practitioner. This has led the Australia Government to develop a new National Medical Workforce Strategy, aiming to address the lack of planning for rural workforce identified over the past 2 decades [1,3].
The 2019 review of studies reporting on Australian undergraduate rural immersion programs resulting from the Rural Health Multidisciplinary Training scheme incorporated data from 19 medical schools that have extended rural clinical placements in their curricula and attempted to determine their effectiveness [4]. Overall, factors most consistently associated with an increased likelihood of rural practice were rural background and rural immersion [4]. For example, these factors predicted rural postgraduate work in a Western Australian cohort, suggesting that students with a rural background were 4 times more likely and RCS students were twice more likely than their metro background counterparts to practice rurally [1]. Other Australian and overseas universities reported similar findings [3,5]. Rural placement experience during medical school has also been reported to positively associate with the intention to live and practice medicine in rural locations [1]. It was also suggested that financial support (e.g., rural bonded scholarships) and the type, quality and duration of rural experience are also key considerations impacting the intention to work rurally [6]. To increase the number of medical students coming from rural locations medical schools often have lower requirements in the main entry requirement selection tools (i.e., the Australian Tertiary Admissions Rank and the Undergraduate Medical and Health Services Admissions Test [UMAT]) for rural entry pathways [7]. This raised concerns that this creates a selection bias towards a less capable workforce coming from and later going to rural areas to service the higher demands of the rural population [8].
This study focuses on factors predicting final year medical students’ intent to practice medicine in rural Australia as well as factors predicting medical school graduates’ employment in rural Australia.
2. Objectives
The objective of this research was to identify the factors that predict two separate outcomes: medical students’ intent to work rurally and graduates’ current employment location. By determining the predictive factors for rural intent and rural employment, the results could be used to further identify incentives, recruitment patterns, policies, or university services that are impacting the workforce shortage faced by rural communities in Australia and globally.
Methods
1. Ethical statement
Ethics approval for this study was granted by the Human Research Ethics Committee of University of New South Wales in 2011 (ref: HC112229) and renewed in 2016 (ref: HC16572). Confidentiality and anonymity of survey respondents was maintained throughout by removing identifying information prior allowing investigators access to the data. Participants’ consent was deemed by responding to questionnaire, which was voluntary.
2. Study design
This is a quantitative observational study utilized data obtained from the UNSW Rural Clinical School and results from the “Destination Rural” questionnaire.
3. Setting
Data were gathered from UNSW students and graduates who had studied for one or more academic year at an RCS campus. The survey was conducted between 2012 and 2017, and respondents were asked to complete the same questionnaire every 2 to 3 years. For this study the most recent survey responses were collated (2015–2017) to establish two distinct populations: students and graduates. The survey was administered by the rural administration staff who posted the questionnaires to all students and graduates who had studied in the rural campuses using the address record available at the administration offices at the time.
4. Participants
UNSW students and graduates (males: 118 [37%]; females: 201 [63%]) who had studied for one or more academic year at UNSW rural clinical campus between 2012 and 2017.
5. Variables
1) Outcome variables
The outcome variables are the intention to work in a rural location after graduating for students and the location of current employment for graduates. These variables were recoded to rural/none rural based on ASGS-RA postcode classification.
2) Data sources/measurement
All variables include data received from the survey. The questions’ face validity is deemed appropriate since these are factual questions [9].
The survey questions include general demographic variables as well as factors related to rurality. Measurement of perceived importance and influence of external factors on employment intention or location such as partners jobs, altruism, and lifestyle were done by 5-Likert scales (all these data were anonymized prior to being provided to the researchers).
Assessment data such as UMAT scores and major academic and clinical assessment outcomes within the medicine program such as weighted average mark (WAM) and objective structured clinical examination (OSCE), which were transformed to standardized scores (mean± standard deviation, 50±10) prior to being provided to the researchers to maintain anonymity.
6. Bias
Due to missing data, potential predictors with more than 10% missing values were excluded from the analysis. This may limit the breadth of the analysis by the exclusion of variable which potentially could increase the variance explained (R2). However, including more variable with larger missing values would decrease the sample size being analyzed. Alternatively, imputing date for the missing values when the missing values are >10% increases the risk of increased impact of unknown bias on the results. Thus, the conservative approach taken is deemed reasonable and valid.
7. Study size
The study used up to 11 predictors in multiple logistic regression, which requires at a bare minimum 55 participants based on the 1:5 ratio or 110 participants based on 1:10 ration based on the desirable minimum sample size [10]. The sample of this study exceeds the two thresholds.
8. Statistical methods
After removing potential predictors with more than 10% missing values, two distinct logistic regression models (backward stepwise method) were established to separately analyze students and graduates using their intention to work rurally and their current employment location as the dependent outcome measures, respectively. All data management and analysis were undertaken using IBM SPSS ver. 26.0 (IBM Corp., Armonk, USA).
Results
1. Participants
The analysis included 131 students between the ages of 22–39 (35.8% males) and 100 students (76.34%) had a rural background, defined as being rural (ASGS-RA 3-5) but only 52 (39.69%) were bonded to work rurally postgraduate at the time of the survey. All survey respondents had completed their final 2 years of a 6-year undergraduate medical program at an RCS campus. The dependent variable was the student’s reported intention to work in a rural location or not (1, 0). Table 1 lists the variables initially considered and those dropped off in the stepwise process.

List of Variables Trailed in Logistic Regression of Students Intention to Work Rurally
2. Main results
The final model for intent explained 30.4% of the variance in the outcomes (r2=0.304) (Table 2). The results demonstrated that the factors that significantly predicted the outcome were having a rural background (odds ratio [OR], 7.16; 95% confidence interval [CI], 2.59-19.53), choosing to study at the RCS (OR, 8.72; 95% CI, 1.32-57.63), and perceiving rural areas as preferred places for opportunities to advance their career (OR, 1.69; 95% CI, 1.15-2.49).
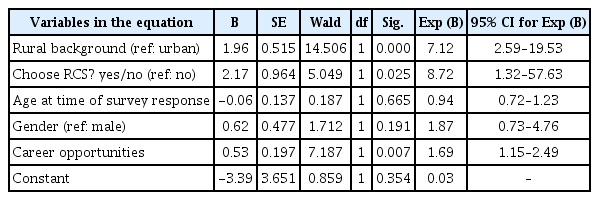
Final Step in Logistic Regression of Students Intention to Work Rurally
A total of 87 graduates (41.38% males; age, 22-39 years old) were included in the second model. Fifty-seven (65.52%) had a rural background, and 63 (72.41%) had the intention to work rurally when they were students. All survey respondents had completed their final 2 years of undergraduate study at an RCS campus. The dependent variable used was the individual’s current location as either rural or not (1, 0).
Table 3 lists the variables initially considered and those dropped off in the stepwise process. The final model for rural location explained 21.0% of the variance in the outcome (r2=0.210) (Table 4). The results of this model demonstrated that the factors that significantly predicted the outcome are being bonded to work in a rural location (OR, 6.40; 95% CI, 1.15-35.59) and the importance placed on serving an under-resourced population (OR, 1.91; 95% CI, 1.02-3.57).

List of Variables Trailed in Logistic Regression of Graduates Current Employment Location

Final Step in Logistic Regression of Graduates Current Employment Location
Discussion
1. Key results
This study aimed to determine the key factors predictive of a student’s intention to work rurally and additionally which factors are predictive of a graduate’s current employment location. There are key differences between these two groups (students and graduates). While student intent is predicted by having a rural background, choosing to study at an RCS and perception of rural areas as having a positive impact on career opportunities (Table 2), a current rural workplace location among graduates is predicted by holding a bonded medical position and a desire to serve an under-resourced population (Table 4).
2. Interpretation
Students with rural background as well as those whose chose to study at an RCS, irrespective of age or gender were more likely to have the intention to work rurally (Table 2). This supports the notion that there is continued value in maintaining a rural pipeline that selects rural students for medical schools and provides them with opportunities to complete undergraduate rural immersion [11]. This is important since the likelihood of a student maintaining interest may decrease if such pathways are not well established [4]. Consequently, these findings demonstrate that maintaining rural interactions with medical students throughout their medical degree is important to maintain or even strengthen their motivation to work rurally after graduation.
3. Comparison with previous studies
Contrary to some previous studies is our finding that rural background was not a significant predictor of actual rural workplace location, but rather the bonding incentive and the increased altruistic perception of the importance of serving an under-resourced population had the greatest impact on rural employment (Table 4) [4]. This suggests that strengthening the associations between rural employment and other personal and psychological traits may enhance that graduates’ inclination to work rurally [12].
An important result of this research is that once in the workforce, different factors are predictive for graduates choosing to work rurally from those that predict their student counterparts’ intentions. This raises the importance of maintaining a longitudinal strategy aiming to encourage and support students and graduates to work rurally throughout their medical training [13]. That strategy should comprise: (1) rural experience during the medical school training; (2) financial incentives (e.g., MRBS); (3) engagement with the rural community to enhance the awareness of the rural communities’ needs; and (4) provision of career development opportunities in rural areas to enable graduates to fulfil their both altruistic values as well as their professional needs.
It is noteworthy that neither academic nor clinical proficiency (WAM and OSCE results, respectively) predict either intention to work in, or employment at, rural areas. This is important since the admission threshold for the rural pathway is lower than the mainstream domestic pathway [14], whereas performance in the medicine program has been proved to be similar across these two admission pathways and as good [8]. This is important evidence suggesting that the graduates from the rural admission pathway as good doctors as their non-rural counterparts.
4. Limitations
Like every study, this one has several limitations. First this study includes a few snapshots of data rather than a longitudinal follow-up of individuals. This limitation is a result of the ethical requirements for collecting unidentifiable, anonymous data which did not allow us conducting that follow-up at the individual level. Consequently, further robust longitudinal research is required to clarify the changes that occur in attitude towards practice in rural areas as students transition to become doctors. The second limitation of this study is the lack of data on Aboriginal and Torres Strait Islander students and graduates as only one of the survey participants identified as Indigenous. Future research particularly looking into rural pathways for Indigenous students is recommended. The third limitation of this research is that some of the variables in the dataset had large proportions of missing data, hence excluded from the analysis. Consequently, some caution is needed when considering the results of this study.
5. Generalizability
This study identified the need to look at and understand the longitudinal dynamics of enhancing medical and healthcare workforce in areas of need. It became clear that factors impacting student intentions to work in rural areas are different from factor actually attracting graduated to work and live there. Therefore, further research into this topic should take a longitudinal approach to better understand how factors impacting employment in rural areas (or any other areas of need) change throughout and post the medical and any other health professions training.
6. Suggestions
Effective interventions aiming to enhance medical and heath workforce in rural and areas of need should not be limited to a particular stage of the training but rather a comprehensive coordinated strategy should take place. Such strategies need to consider professional, societal, cultural, and financial needs of students and graduates to maintain the attraction of working in such areas of need, from the first day in the medical or health professions school through to professional lifetime career.
7. Conclusion
Overall, this study provides additional insights that have the potential to enable the revision and implementation of informed policy guidelines, incentives, and university procedures to further improve the outcomes of medicine programs aiming to achieve both professional and societal objectives. In particular terms, the insight from this study may help create a future which sees equitable geographical distribution of doctors, thereby improving the health and wellbeing of rural Australians and rural populations in other countries facing similar challenges.
Acknowledgements
Staff of the University of New South Wales Rural Clinical Schools are thanked for their logistical contribution to the administration and distribution of the questionnaire, and the author is grateful to all students and graduates of the University of New South Wales medical program who voluntarily participated in the survey.
Notes
Funding: No financial support was received for this study.
Conflicts of interest: No potential conflict of interest relevant to this article was reported.
Author contributions: Conceptualization: LF, BS; data curation: LF, CG; formal analysis: CG, PH; methodology: BS, LF, PH; project administration: CG; writing–original draft: CG, PH, BS, LF; writing–review & editing: CG, PH, BS, LF.