Flipped clinical training: a structured training method for undergraduates in complete denture prosthesis
Article information

Abstract
Purpose
To design and implement flipped clinical training for undergraduate dental students in removable complete denture treatment and predict its effectiveness by comparing the assessment results of students trained by flipped and traditional methods.
Methods
Flipped training was designed by shifting the learning from clinics to learning center (phase I) and by preserving the practice in clinics (phase II). In phase I, student-faculty interactive session was arranged to recap prior knowledge. This is followed by a display of audio synchronized video demonstration of the procedure in a repeatable way and subsequent display of possible errors that may occur in treatment with guidelines to overcome such errors. In phase II, live demonstration of the procedure was given. Students were asked to treat three patients under instructor’s supervision. The summative assessment was conducted by applying the same checklist criterion and rubric scoring used for the traditional method. Assessment results of three batches of students trained by flipped method (study group) and three traditionally trained previous batches (control group) were taken for comparison by chi-square test.
Results
The sum of traditionally trained three batch students who prepared acceptable dentures (score: 2 and 3) and unacceptable dentures (score: 1) was compared with the same of flipped trained three batch students revealed that the number of students who demonstrated competency by preparing acceptable dentures was higher for flipped training (χ2=30.996 with p<0.001).
Conclusion
The results reveal the supremacy of flipped training in enhancing students competency and hence recommended for training various clinical procedures.
Introduction
Competency in any particular clinical skill requires mastering an explicit set of subcomponents related to the procedure and so professional care for a patient when it is performed. Clinical training supports a trainee student to attain a required level of skills to perform a procedure competently and independently in a clinical environment. Skills such as history taking, examination of a patient, effective communication and professionalism are best learned in the clinical environment setting. In the case of learning an interventional procedure or procedures with series of steps that require patients cooperation for complex functional movements are unique problems in clinical teaching that demands to restructure the training approach. The problems in existing observational method of chair side/bedside learning are the lack of provision for observing possible errors and how to overcome such errors. The demonstration given by an experienced clinical teacher focuses only on the accurate steps and is similar to bookish learning. The emphasis on patient-centered care, professional integrity in clinical education and students assessment, faculty clinicians are expected to practice a range of teaching skills [1]. Teaching plan with precise structure and supporting sources can bring about encouraging results in teaching quality and students competency. A flipped teaching is one such pedagogical method in which the teaching elements of a course are reversed. Flipped clinical training as similar to flipped classes, restructure the training pattern. In flipped classes, the students need to learn the text by using prerecorded lectures at home and class hours are used for interactive discussions or projects to apply the knowledge [2]. In flipped clinical training, students learn about the procedure using interlinked learning activities, assessments and feedback in clinical center whereas clinical hours are used to practice the learned skill. So it reallocates the training from observation and movement repetition to structured learning and competent performance.
Fabrication of functionally acceptable removable complete denture is a challenging task for even experienced dental practitioners and undeniably a hard-hitting for beginners. Undergraduate students training in treating completely edentulous patients by functionally acceptable removable complete dentures need to be addressed with a more systematic approach. In Indian dental schools preclinical and clinical teaching are carried out by a prefixed number of exercises to train our graduates with the assumption that the students’ skill will be enhanced by practice. Although the competence needed in complete denture prosthesis is multilayered and requires diligent practice, sub-skills which span between the boundaries of an initial examination to post denture insertion need to be taught with a clear outline of tasks and assessed periodically to construct the final core competency as an achievable target. In the existing training method, learners are getting their hands on skill by “modeling,” which means observing and imitating actions carried out by the clinical instructor (model) and then they will try to accomplish the task by “movement repetition” [3]. In this observational learning method, the student is focusing on actions without a clear theoretical framework, and the instructor may not be code the actions in a repeatable way. When students start performing the task, they make errors at different phases and correcting with instructors support which results in slow and incremental learning. When a situation requires an alternate or additional action that has never before been demonstrated, then the concept of repetition will not support the performance. Hence there is a requirement for developing structured training activities and assessment methods to replace the traditional chair side training. The medical literature review also supported our concept that structured methods aiming to teach novice have led to sustained improvements in self-reported confidence [4,5].
Student dentists are invariably struggling to demonstrate competence in complete denture treatment (highly individualized treatment that requires tracking jaw movements with remarkable precision to optimize oral health by replacing all missing teeth). Therefore, we aimed to design and implement a pilot project on flipped method for complete denture training to provide a comfortable learning environment for the novice learners and systematically train them to reach the expected level of competency.
Subjects and methods
Analytical type of observational study was conducted on flipped training method in complete denture treatment in Faculty of Dental Sciences, Sri Ramachandra University, India, in the period between 2013 and 2016. Convenient sampling technique was used to recruit the subjects. Approval was obtained from Institutional Review Board as a part of “competency-based clinical dental education” project. The study population is final year undergraduate dental students (Batch I, n=60; Batch II, n=59; and Batch III, n=62) and were introduced to clinical side following 40 hours of lecture classes, 80 hours laboratory training and studio trained (teacher to student ratios of 1:6) to treat patients with completely edentulous maxillary and mandibular arches using removable complete dentures. To enhance students competency by minimizing the errors and capitalizing their efficiency, we flipped our training approach in two phases as an amalgamation of learning the cognitive and motor components of the skill and performing the skill (Table 1). Phase I training was carried out in the clinical learning center using audio synchronized video demonstration of the procedure performed by a faculty clinician on a standardized patient in a precise manner. This allowed students to learn at their own pace with an adequate number of times as per individual need. This is followed by another video demonstration of the procedure which focused on all possible errors that tend to happen during the procedure and directions to overcome such errors. Phase II was organized in a clinical environment with the demonstration to observe the process in a real environment and followed by training students to perform on patients under faculty clinicians observation. Students were made aware of the purpose of new training method by concerned faculty members before implementation. Students concerns about faculty support, time limit, and differences at individual levels in qualifying the formative exams were addressed and assurance was given within realistic limits. Fig. 1 reveals the program details of phase I [6,7,8,9,10] and phase II [11,12].
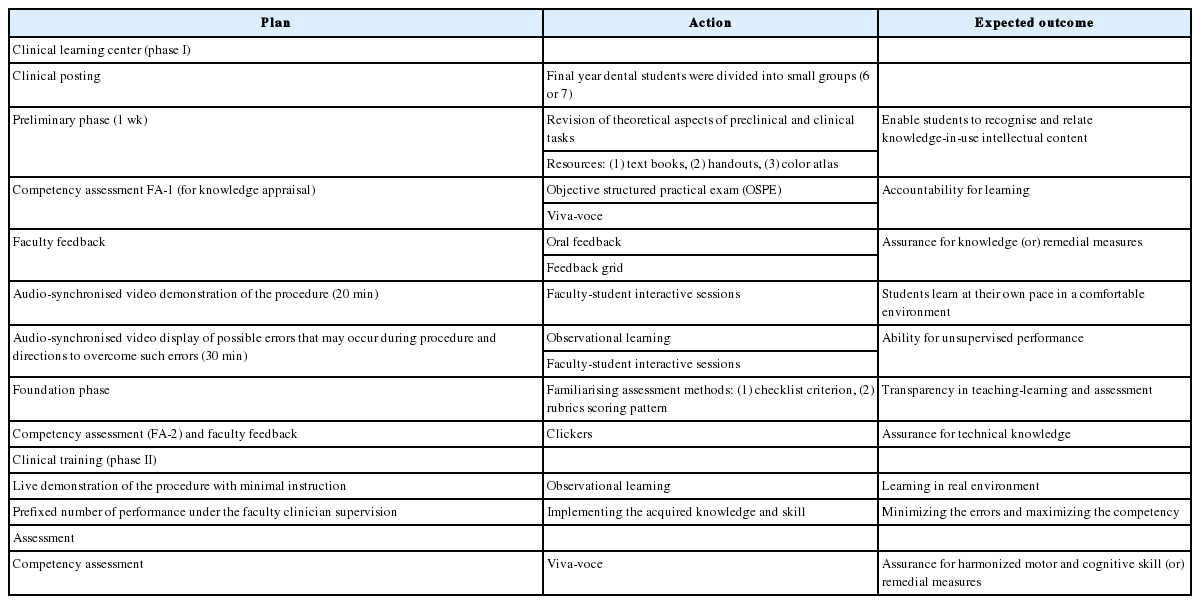
Flipping Framework
Program Plan for Complete Denture Training in Flipped Method
With this training, students treated three different patients who are completely edentulous with instructor’s guidance and stepwise monitoring. Instructors also shared how they will be assessed based on a checklist criterion [13] and rubrics [14] in assessments.
To measure the teaching–learning outcome, students were subjected to summative clinical examination to assess their competency in treating edentulous patients with aesthetically and functionally acceptable dentures. Students independently performed the clinical and laboratory works. Two examiners assessed each candidate based on the checklist criterion and rubrics for grading their work. Results were summarized for outcome evaluation. We started adopting this clinical training method and assessment technique for the subsequent year students and totally three batches of student completed this method of training and analyzed (Batches I, II, and III). Upon considering the summative result as a supporting document for evaluating the outcome, we reviewed the results of three consecutive academic batches (control group students: Batch A, n=57; Batch B, n=63; Batch C, n=60, between 2010 and 2013, who were trained by traditional method of clinical teaching but assessed using the same checklist criterion and rubric method) and compared with three batches (Batches I, II, and III) trained by flipped method. Tables 2 and 3 illustrate the checklist criterion and rubric scoring method (score 1 for unacceptable dentures with major errors, score 2 for acceptable dentures with minor errors that do not compromise outcome, and score 3 for acceptable dentures with no evidence of errors) followed in both traditional and flipped methods.

Individual Observation Checklist for Competency-Based Assessment in Removable Complete Denture Treatment

Rubrics Used for the Assessment of Complete Dentures
We invited the same internal examiners who assessed the control group students to assess the study groups also. The examiners a had clear understanding about different training modes and the potential for variability between subjects in performance hence agreed with each other to apply the same assessment protocol that was used for the control groups so as to bring fairness in assessing the specific component skills. The collected data was analyzed for knowing students competency in preparing acceptable dentures by applying chi-square test using SPSS version 20.0 (IBM Corp., Armonk, USA) to find out the statistical significance.
Results
We considered the traditionally trained three batches and the flipped trained three batches for statistical analysis. This was done by clubbing the score 2 and 3 (dentures with minimal errors that needs minimal corrections for acceptance and acceptable dentures that needs no corrections) as one group and score 1 (unacceptable dentures) as another group (Fig. 2). Results showed that the number of students who demonstrated competency in complete denture treatment was more for flipped training method and hence has high statistical significance (χ2 value 30.996 with p<0.001) than the traditional method.

Comparison of Number of Students Preparing Acceptable and Unacceptable Dentures among the Study (Flipped) and Control (Traditional) Groups
A total number of students who demonstrated competency by preparing acceptable dentures with no evidence of errors and dentures with minor errors that can be corrected (scored 3 and 2) and total number of students who demonstrated incompetence by preparing unacceptable dentures with major errors (scored 1) among study and control groups.
Competency of students in treating completely edentulous patients trained by both methods is shown in Fig. 3 by displaying the percentage of students scored 1, 2, and 3. The increase in the percentage of students who scored 3 in flipped method clearly reveals its supremacy in training efficiency.
Comparing the Effectiveness of Traditional and Flipped Training Method by Projecting the Percentage of Students Scored 1, 2, and 3
Batches A, B, and C: Traditional training; Batches I, II, and III: Flipped training.
Discussion
Imparting practical skills is a diligent task in dental education and teaching the skills in a clinical environment is even more complex. In this study, we intended to train our undergraduates to achieve competency in treating completely edentulous patients by removable complete dentures by flipping the clinical learning and clinical practice. The training environment maximized the learning opportunities by using specifically designed sessions (Fig. 4) that covered the cognitive segment (identification and development of the component parts of the skill), and associative segment (connecting the component parts into action) in phase I and autonomous segment (practicing the learned skill) in phase II. This arrangement was discussed in detail with students before they were introduced to the newer approach and prepared them to engage in learning activities.

Template for Flipped Training
Cognitive and technical aspects are essentially needed to be merged in skill learning but invariably they are happening at different environment (lectures and discussion) and at varying time sequence. In dentistry, students spend most of their learning time in prosthodontic laboratories during preclinical period hence adapting easily to lab related works in denture fabrication but their clinical activities need to be fine-tuned by integrating preclinical theory knowledge to the basic steps. If there is uncertainty, incompleteness or flaw in prior knowledge, it deters the quality of clinical performance. In traditional training method, students experienced difficulty in performing the skill after observing the demonstration of the experienced clinician as they are making an errorless performance. When students try to repeat their observed learning, they are experiencing the technical hitches of normal anatomical variants, functional habits, and patient’s cooperation. Merely instructing the ideal steps and observing the expert’s demonstration in traditional method set hurdles for the students to overcome such realistic situations in treatment care. The video recorded demonstration of possible errors helped our learners to get ideas about the various situations they need to handle and what they will neglect or over-enthusiastically perform in the course of action. Recall sessions and discussion between the faculty clinician and students during a demonstration is the concept reflection of building new knowledge on existing knowledge. This inspired our study group students to internalize the purpose of every action and actively participate in the learning program.
Students performance are largely influenced by the amount of deliberate engagement in their training program. In the traditional method, deliberate engagement is as same as rote repetition and no chance for learning the way to solve the real problems. In flipped training, students were familiarized with the anticipated problems and taught to solve the problem before executing the skill. This approach promoted an understanding of refreshing the existing knowledge and repeated learning to acquire a new skill. Appropriate integration of audiovisual aids added a new dimension to learning by overcoming the difficulties in grasping the interconnected steps involved in a complex procedure and get familiar with what learning is supposed to achieve.
Unaccepted performance due to students inherent inabilities in the psychomotor domain is a critical issue in any training program and same happened in our case. In the study group, 13%, 7%, and 15% of students in batches I, II, and III demonstrated their incompetence (scored 1) though the value is comparatively less than the traditional training (47%, 25%, and 38%). Another remarkable finding to be noted in our study is the lack of considerable difference between the percentage of students scored 2 (an acceptable level of competence) in two training methods and this need to be addressed in future for a promising outcome.
The clinical learning center in flipped method provided students with a safe and shielded atmosphere to learn the procedure until they become confident to enter the clinic and perform in a patient. Patients visiting university hospitals are often offended by the quality of care provided by student dentists during the learning phase as they have no experience. Patient’s expectations and attitude frequently affect the learning especially when there is a need to correct the procedure for bringing the intended quality [15]. Flipped training optimizes students knowledge and familiarization of the procedure before they start treating patients and thereby increase their level of competence.
The multiple formative assessments in flipped program were tailored to meet the specific requirement and encouraged learners for self-improvement, motivated to achieve the next level, and placed values at every aspect of the procedure [16,17]. The assessment results and students involvement helped our faculty members to recognize and develop teaching–learning methods based on needs and “what will work” for their current situation and not too confined to the boundaries of tradition.
The study model and assessment results concludes that flipped method is an effective clinical training model for students in terms of learning clinical skills, acquiring adequate knowledge background, developing the ability to self-analyze the aptness of every step, and confidence in providing independent treatment. The flipped training reversed the flaws in traditional training and included effective elements to facilitate cognitive skills merged with technical skill that improved the overall performance of students. However, this training method was piloted for a single procedure and the universal acceptance depends on the design and implementation for different procedures with varying level of complexity in future.
Acknowledgements
We would like to thank Dr. M. Umamaheswari, Department of Prosthodontics, Sri Ramachandra University for her active involvement and technical support in this work.
Notes
Funding
None.
Conflicts of interest
None.