Introduction
Doctors solve complicated problems by interacting with patients, patient’s families, and other specialists. Complexity experienced in clinical practice requires not only clinical reasoning, scientific reasoning, and skilled action but also personal reflection [1]. Reflection refers to carefully reflecting on and thinking about one’s experiences, actions, feelings, and reactions and analyzing and interpreting them to learn from them [2]. Reflection is done not as temporary thinking but as a process, and the process of reflection leads to insight [3], which is gained by discovering and restructuring an overall problem situation [4].
Insight clarifies one’s thoughts, emotions, and actions [5] and helps an individual develop a new understanding by exploring one’s experiences [6]. The reflective activity contributes to professional identity development by promoting an understanding of the beliefs, attitudes, and values individuals must have in the vocational environment and cultural context and cultivating the capacity to accept them comprehensively [7,8]. It also helps establish an integrated foundation of professional knowledge by contributing to the connection between existing and new knowledge. In particular, reflection is an essential foundation for developing vocational professionalism in self-regulation and management by having individuals monitor themselves and be aware of their problems [9].
Reflection is necessary for developing professional competencies and enabling insightful thinking in medical situations. Schön [10] introduced reflection as a tool for re-experience in which experts solve complex problems related to jobs and learn in the process and suggested the concept of “reflective practitioner.” Experts tend to be self-reflective, by which they understand and analyze the overall flow of a problem, find the best solution, and practically and autonomously utilize the solution. They use self-reflective thinking as a valuable tool to learn from experience and outline complex problems. Reflective thinking and practice form the basis of expert knowledge and can be practical tools for solving complex problems in specialized fields.
Reflection, especially personal reflection on experience, is a key factor for acquiring and maintaining balanced professionalism along the continuum of medical education [11-14]. Students with higher levels of reflection find more benefits and pleasure in their learning, show better academic performance, earn higher scores in diagnostic thinking during clinical training, and increase efficiency [15] and autonomy in self-regulated learning [16]. Reflection and reflective activity are very effective in developing and maintaining doctors’ professionalism and practical competence [6,7,17,18].
A reflection tool for doctors and medical students has already been developed because of its importance [5, 16,19,20]. The Self-reflection & Insight Scale (SRIS) developed by Grant et al. [5] measures individuals’ self-awareness, and the scale developed by Sobral [16] measures reflection in a learning situation in a medical program. Aukes et al. [1] developed the Groningen Reflection Ability Scale to assess personal reflection in medical science, which includes three categories: selfreflection, empathic reflection, and reflective communication. The scale developed by Mamede and Schmidt [20] is a questionnaire mostly on reflection during medical diagnostic reasoning, which covers various aspects of reasoning such as openness and tendency to create multiple alternative hypotheses, the will to reflect on other hypotheses and one’s assumption, and the will to test their hypotheses. However, many existing reflection tools are focused on different perspectives, measuring the reflective characteristics of only one field.
To solve this problem, Priddis and Rogers developed the Reflective Practice Questionnaire (RPQ) that evaluates the extensive psychological structure of reflective practice [21]. The RPQ comprises substructures such as “reflectionin-action,” “reflection-on-action,” “reflection with others,” “self-appraisal,” “desire for improvement,” “confidence (general),” “confidence (communication),” “uncertainty,” “stress interacting with patients,” and “job satisfaction.” “Reflection-in-action” indicates instantly occurring reflection, and “reflection-on-action” indicates reflection on incidents in the past. One of the factors of the RPQ is communication with the patient. It includes various fields of reflection experienced by doctors in a medical environment. It assumes that personal reflection and the tendency to reflect on others may increase reflection on one’s capacity.
However, despite the emphasis on the importance of reflection for doctors, there is insufficient research in Korea on the development of tools to measure the reflection of doctors. In particular, no multilateral reflection tool has been developed for communication with the patient in clinical clerkship. The current RPQ was developed and validated for use in other countries, but its reliability and validity have not been confirmed in the context of the Korean medical situation.
Therefore, this study aims to translate the RPQ developed by Priddis and Rogers [21] into Korean and develop the Korean version of the RPQ (K-RPQ) by testing its reliability and validity. Based on the result, develop a reflection scale to measure the reflective characteristics of medical students in Korea.
Methods
1. Research design
The RPQ was translated after obtaining approval from Priddis, the lead author and original developer. The tool was developed to evaluate psychological constructs related to reflective practice in an extensive context with reflective supervision. This tool includes 10 subfactors, each comprised of four items (total 40 items): reflectivein-action, reflective-on-action, reflective with others, self-appraisal, desire for improvement, confidence (general), confidence (communication), uncertainty, stress interacting with clients, and job satisfaction. Cronbach’s α of each subfactor ranged from 0.666 to 0.919. The RPQ items are primarily focused on interaction with clients. Still, this study translated the RPQ focused on the interaction between students and patients to use the tool in clinical clerkship situations at medical school. First, the researchers translated the English version into Korean. Then, two professors fluent in both Korean and English with experience in clinical clerkship education compared the translated items with the original version and reviewed and discussed whether the expressions and choice of words were appropriate, whether the context and meaning were well delivered, and whether there were items requiring revision due to cultural differences. One bilingual clinical professor proficient in English and Korean backtranslated the tool and reviewed whether there were any distortions in meaning compared to the original tool. Next, two medical students evaluated, from the student’s perspective, whether the terms used in each item were ambiguous, unclear in meaning, or difficult to answer. Their opinions were gathered to complete the Korean version of the questionnaire ultimately. As in the original tool, each item was rated on a 6-point Likert scale (extremely=6 points, not at all=1 point), with higher scores indicating higher reflective capacity.
2. Research participants
This study was conducted on 87 junior (43.1%) and 115 senior (56.9%) medical students with clinical clerkship experience in seven from November 2021 to February 2022. The participants included 113 male (55.9%) and 89 female students (44.1%).
3. Research tools
To investigate the criterion validity of the K-RPQ, we investigated the correlations with the PRQ and other questionnaires. For example, we used “the Korean Self reflection and Insight Scale (K-SRIS),” which measures the attitude of daily insight, and “the Reflection-in-Learning Scale (RinLS),” which measures students’ reflective learning experiences in medical school. And we tried to find the correlation between clinical performance self-efficacy and RPQ using “The Self-efficacy in Clinical Performance Scale (SECP).”
1) Korean Self-reflection and Insight Scale
The K-SRIS used by Song and Kim [22] on nursing students were used to test the criterion validity of the K-RPQ. This tool is a self-report questionnaire consisting of 16 items in two subfactors: self-reflection (11 items) and insight (five items). Only the self-reflection scale was used in the study. Cronbach’s α was satisfactory at 0.875. Example questions for self-reflection include: (1) It is important to me to try to understand what my feelings mean; (2) It is important to me to be able to understand how my thoughts arise.
2) Reflection-in-Learning Scale
The RinLS developed by Sobral [16] for medical students was used to test the criterion validity of the K-RPQ. This tool has a single factor that consists of 14 items in the form of a self-report questionnaire. The tool was rated on a 7-point scale, with higher scores indicating higher reflection-in-learning. Cronbach’s α in this study was very satisfactory at 0.923. Example questions for RinLS include: to what extent have I: (1) carefully planned my learning tasks in the courses and training activities of the medical program; (2) talked with my colleagues about learning and methods of study.
3) Self-efficacy in Clinical Performance Scale
The SECP used by Park [23] on medical students and interns was used to test the criterion validity of the K-RPQ. The SECP comprised 36 items in seven subfactors: knowledge acquisition and application (six items), clinical reasoning (seven items), clinical skills (six items), communication with patients (six items), relationships with other health professionals (four items), medical ethics (five items), and self-development (four items). Cronbach’s α of each subfactor in this study ranged from 0.723 to 0.868. Higher scores for each factor indicated higher efficacy. Example questions for SECP include: (1) I constantly strive to learn new medical knowledge or skills (self-development); (2) I am able to appropriately elicit medical histories related to their care and treatment from patients (communication with patients).
4. Data collection method and ethical considerations
Data were collected from November 2021 to February 2022 from junior and senior medical students from seven medical schools on Google online survey. Students who read the information of informed consent and voluntarily agreed to participate responded to the survey through the online survey link (Google Form) provided in the notice. The adequate sample size recommended for exploratory factor analysis is at least 100 samples [24], and the sample size necessary for confirmatory factor analysis is at least 150 [25]. The number of samples we collected met this requirement. It took approximately 20 minutes to complete the survey. Of 205 copies of the questionnaire that were collected, 202 were used in the final analysis, excluding invalid responses. This study was approved by the Gil Medical Center Institutional Review Board of Gachon University (IRB approval no., GCIRB-2021-448).
5. Analysis method
Data analysis was conducted by testing the validity and reliability of the validated RPQ tool by Priddis and Rogers [21] domestically. The construct and criterion validity of the instrument was tested. Construct validity was tested using exploratory factor analysis and confirmatory factor analysis. The common factor model was conducted for exploratory factor analysis, and a direct oblimin rotation was used for factor rotation. The suitability of factor analysis was tested by Bartlett’s test of sphericity and Kaiser-Meyer-Olkin (KMO). The maximum likelihood method was selected to estimate the coefficients of the model in confirmatory factor analysis, and the fit of the factor structure model was determined using χ2/degrees of freedom (df), Tucker-Lewis index (TLI), comparative fit index (CFI), and root mean square error of approximation (RMSEA). To verify the relationship between a specific criterion and this tool, criterion validity was analyzed by calculating Pearson’s correlation coefficients with the K-SRIS, RinLS, and SECP. Cronbach’s α was conducted to test the reliability of the K-RPQ.
Results
1. Validity
1) Construct validity
a. Exploratory factor analysis
To test the normality of the data used in the present study, the skewness and kurtosis of each item were analyzed (Table 1). According to the criterion of Kline [26], if the criterion for skewness does not exceed the absolute value of 3 and the criterion for kurtosis does not exceed the absolute value of 8, it can be regarded as a normal distribution. Therefore, this study is the acceptable range of skewness and kurtosis for normal distribution of data.
The KMO of the data is 0.856, and Bartlett’s test of sphericity showed the following results: 5,044.337, df=780, p<0.001, proving that the data were suitable for factor analysis. There was one item with a commonality of 0.40 or below (D14). Thirty-nine items were finally extracted, excluding one item classified as a conceptually different factor compared to the original scale in factor analysis. There were 10 factors with eigenvalues exceeding 1.0, and the total variance was 71.88%. The items of each subfactor were categorized in the same way as the original scale. Self-appraisal comprised three items because one item (D14: I think about my weaknesses in working with patients) was excluded (Table 2). Each factor was named the same as the original scale.
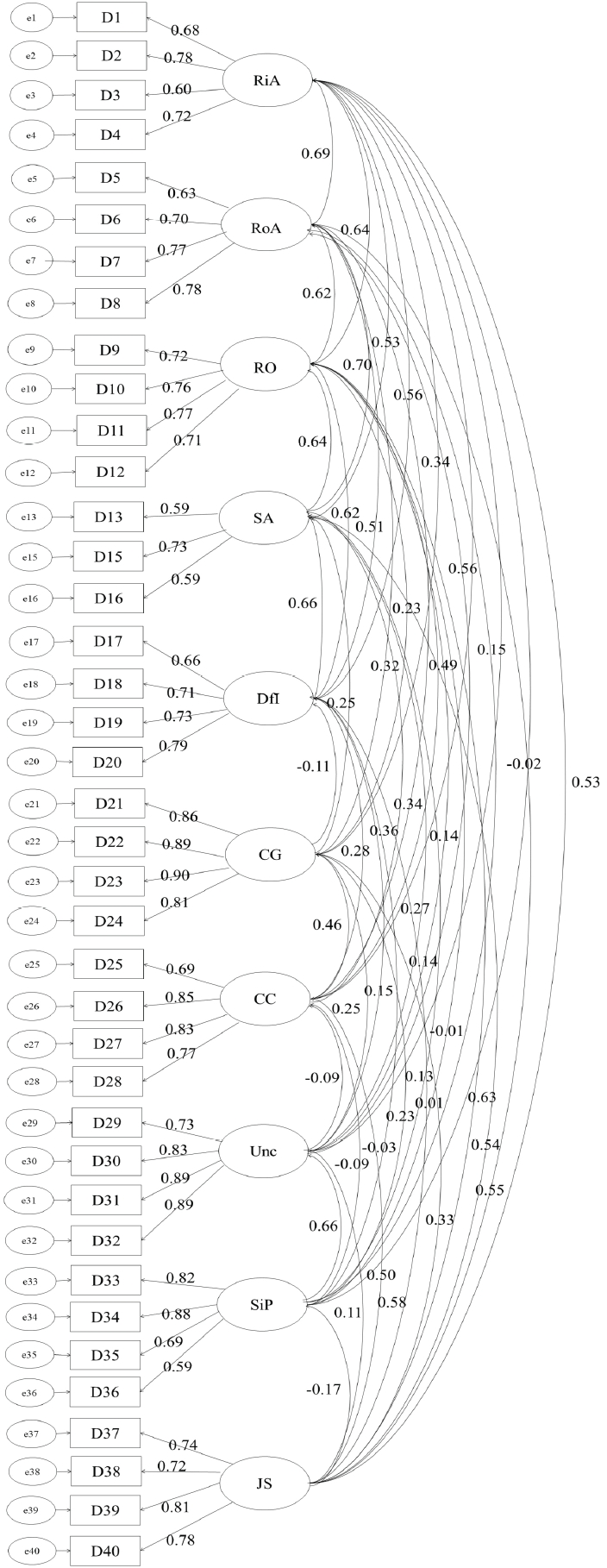
b. Confirmatory factor analysis
Confirmatory factor analysis was conducted to test the fit of the 10 factors extracted in the exploratory factor analysis. The result of testing the model fit was χ2=1.980 (df=657, p<0.001), thereby significant. The fit indices of the model were CFI=0.859, TLI=0.841, and RMSEA=0.070 (90% confidence level, 0.064–0.075). Each index was acceptable, proving the model’s fit, and no item was deleted (Fig. 1).
2) Criterion validity
For criterion validity, this study examined Pearson’s correlation coefficients between the K-RPQ and the subfactors of the K-SRIS, RinLS, and SECP (Table 3). Most subfactors of the K-RPQ showed a positive correlation (r=0.219–0.559) with other reflection scales, such as the K-SRIS and RinLS. However, stress interacting with patients (subfactor of the K-RPQ) showed a negative correlation (r=-0.231) with self-reflection (subfactor of the K-SRIS). Among the K-RPQ subfactors, eight, except for uncertainty and stress interacting with patients, showed a positive correlation (r=0.140–0.637) with all factors of the SECP.
2. Internal consistency reliability and intercorrelations among K-RPQ sub-factors
Cronbach’s alpha values ranged from 0.666 to 0.919, which are generally satisfactory. The confidence (general) (mean± standard deviation [SD]=2.99±1.30) was the lowest among the K-RPQ subfactors, and the desire for improvement (mean±SD=5.22±0.73) was the highest. The general pattern of the inter-correlations among K-RPQ subfactors showed a positive correlation (r=0.160–0.597) (Table 4).
Discussion
This study aimed to translate the RPQ developed by Priddis and Rogers [21] to produce a Korean version of the reflection scale (K-RPQ) for clinical clerkship of medical students. As a result of the exploratory factor analysis of the K-RPQ, 39 out of 40 items were classified into 10 factors, with each subfactor consisting of the same items as the factors in the original RPQ [21].
K-RPQ was composed of 10 sub-factors. For example, “reflection-in-action” occurs while we are working. It involves being aware of our experiences and connecting with our feelings. “Reflection-on-action” appears after the event. Therefore, reflection-in-action refers to reflection occurring at the moment, whereas reflection-on-action refers to reflection on past events. “Reflection with others” includes reflection that might occur with peers or in formal supervision. “Self-appraisal” acknowledges that a tendency for personal reflection and reflection with others likely fosters an increased tendency to reflect upon and question one’s capabilities for practice. The “desire for improvement” sub-scale gauges one’s inclination to further expertise. “Confidence in one’s general ability” is measured via a confidence (general) sub-scale, and “confidence more specifically related to communication” is assessed via a confidence (communication) sub-scale. “Uncertainty” stimulates reflection as one reflects on trying and resolving the uncertainty. Finally, the RPQ contains “stress interacting with patients” and a general “job satisfaction” sub-scales [21].
Moreover, there was high inter-item reliability and correlation, which proved the validity of the K-RPQ for medical students. The K-RPQ validated in this study is expected to be widely used to identify the level of reflection and provide feedback to improve medical students’ professionalism and insightful thinking skills. This study excluded one item (“I think about my weaknesses for working with patients”) from selfappraisal, which differs from the previous research [21]. Medical students tend to concentrate on studying and learning, lacking the sense of responsibility of a doctor. They are in the process of developing themselves by recognizing their weaknesses. This is why they still have difficulties reflecting on their weaknesses. However, as it is crucial to build and maintain therapeutic relationships with patients in addition to having adequate knowledge and skills required of a great clinician, reflecting on one’s weaknesses in patient relationships is a critical factor that medical students must consider in clinical clerkship [27]. In particular, self-appraisal in the RPQ is vital as personal reflection or reflection with others evaluates one’s strengths, weaknesses, and approaches and simulates self-growth [28,29]. Thus, the deleted item on reflection of one’s weaknesses in patient relationships must be studied again later.
Priddis and Rogers [21] reported a strong positive correlation among subfactors such as reflection-in-action, reflection-on-action, reflection with others, and selfappraisal. This study and previous research on the RPQ [21] mostly showed similar relationships, but desire for improvement and stress interacting with patients showed a negative correlation, while “uncertainty” and “confidence (general)” showed a positive correlation. The previous research also showed the highest correlation between “job satisfaction” and “confidence (communication)” [21], but this study did not. This may be because the participants were students, meaning measuring their satisfaction in terms of occupation was insignificant.
The validity of the RPQ on medical students has been tested and confirmed in many previous studies. Priddis and Rogers [21] discovered that the RPQ could identify students who lack confidence, are stressed by interacting with patients, or are unwilling to reflect on themselves. Priddis and Rogers [21] used the RPQ to compare the level of reflection between senior medical students, mental health specialists, and general participants and revealed that medical students showed a higher level of reflection than other participants. In the future, researchers should use the validated K-RPQ to conduct studies on medical students in Korea.
This study was conducted only on medical students in Korea without surveying the general public or those working in other medical fields. Further research with a broader scope comprising medical personnel and the general public will yield more reliable results and confirm the generality of K-RPQ as a self-reflection tool suitable for developing Korean medical personnel and the growth of individual healthcare workers.
This study concluded that the K-RPQ could be used as a self-reflection tool in Korean medical education, as the original version proved in the previous research [21]. This can be applied to program assessments, especially programs aimed at improving students’ reflective skills. Moreover, the K-RPQ can be used in education to fill out students’ self-reflection questionnaires and develop students’ professionalism. Moreover, the results can be used for self-reflection and insight evaluation of medical students in Korea and the development of specific learning strategies, thereby ultimately contributing to improving the quality of education in medical schools.