Introduction
Alumni or medical graduates are among the stakeholders who make an important contribution to assessing the outcome of physicians’ education. As part of the evaluation of educational outcomes, the views and perspectives become essential things to consider. Professional behavior and clinical competence expected of a medical graduate can be a benchmark for the success of an institution in achieving the desired targets and output.
Professional development varies across historical and cultural contexts. Therefore, assessment must consider contextual, cultural, and linguistic specificities, and there is growing literature in these areas to assist medical teachers [1,2]. The achievement of professional behavior is highly related to medicine’s social responsibility, so the definition of it should be refined regularly to reflect the change [3]. Research exploring medical graduates’ perspectives as well as tensions between individual and institutional values concerning clinical competence and professionalism are highly prioritized.
Clinical competence and professional development are two important things that reflect the achievement of medical educational outcomes. One strand of the literature reported the need to explore professionalism in the clinical workplace and examine professionalism across linguistic and cultural contexts [1,4]. Medical faculty University of Islam Bandung has been established since 2005. Medical graduates or alumni are the stakeholders in medical education besides patients, preceptors, medical students, and lecturers. Their perception of clinical competence achievement and professional development in clinical work should be considered, given their experience with the medical program until they start practice in the workplace. Such experience positions them to provide precious input regarding evaluating the success of curriculum delivery.
Patient management can be deemed as a surrogate outcome for test evaluation of patient outcomes [5]. There are some valuable influences on patient management ability namely medical competence, professional behavior, and interpersonal skills.
Medical competence is combining elements of technical ability and knowledge (awareness of and interest in the disease, continuity of follow-up, and requesting specific tests) with interpersonal skills related to communication, information (informing, listening, trust, prompting questions), and attention (courtesy, cordiality, respect, interest, and approachability) [6]. In other words, medical abilities are divided into two categories, namely cognitive competence and clinical skill competence. While interpersonal abilities are inherent self-abilities in individuals in the form of personal attributes and humanism attitudes shown. Professional behavior was defined as a set of qualities and attributes of a person’s behavior that is observable and relates to medical practice [7].
Working as a doctor for at least 3 years has provided enough experience in managing patients. This research was obtained from interviews with alumni who have worked in hospitals [8].
Based on the research problem stated previously, this study aims to identify the most influential factor of medical competence regarding patient management ability under medical graduates’ perspective of Universitas Islam Bandung, Indonesia.
Methods
The design of the study is an analytic observational with a cross-sectional approach. Using primary data, we gather perceptions of medical graduates regarding clinical competence achievement and professional development. Medical graduates’ perceptions will be obtained by distributing the questionnaire of perception that had been validated previously [7].
The study takes place in the Faculty of Medicine from June to August 2022 to Medical School graduates’ batch 2010 until batch 2019 who have met inclusion criteria. They were recruited using a purposive sampling technique. In other words, those who graduated in 2019, when the data was taken in 2022, had been working for 3 years.
1. Study participants
This study recruited medical graduates’ batch 2010 until batch 2019 from the medical faculty of UNISBA, Indonesia those who meet the following inclusion criteria: (1) medical graduates who graduated with long experience for at least 3 years; (2) have participated in an internship program or equivalent program; and (3) those who have practiced as a medical doctor either personally or in a government institution, worked as a lecturer, or continued specialist schooling.
The amount of 206 medical graduates was selected and invited to participate in this study via purposive sampling. The sample size was determined based on an online calculator for structural equation modeling. The calculation is based on the number of six latent variables with 35 observed variables and an anticipated effect size of 25%. The desired statistical power level of 70% and 95% of confidence intervals.
2. Study procedures and instrument
Measurement of the perception of medical graduates is carried out using instruments regarding the achievement of clinical competence and professional behavior, divided into six domains [7]. The fifth components, namely, professional behavior, humanism, clinical skills ability, cognitive competence, and interpersonal skill were utilized as independent variables to influence patient management ability as the dependent variable. Medical graduates’ perspective regarding clinical competence and professional development is a perception in Likert scale form. Participants were asked to score their agreement for each item in the questionnaire on a 5-point Likert scale ranging from 1 (disagree) to 5 (strongly agree) (Supplement 1). The instrument was developed by the author itself in 2020 with three phases of item development (qualitative, item construction, and item validation). This instrument is reliable to other research because it has a very high internal consistency as evidenced by Cronbach’s α of 0.916. The tool has six domains with 35 items consisting of professional behavior (nine items), humanism (seven items), clinical skills ability (six items), patient management (eight items), cognitive competence (three items), and interpersonal skills (two items). This instrument was chosen because it can better describe the characteristics of variables observed in Medical School of Bandung Islamic University, in which the process of preparing the instrument is adjusted to the conditions of graduates in the field and carried out in a systematic manner.
A validity test of the measurement tool was carried out through psychometric properties via exploratory factor analysis on 84 respondents before taking a true survey. The item is stated valid if it has initial communalities >0.7 (t loading factor >1.96). All 35 items were valid based on that result. Reliability is identified by a coefficient ranging from very low coherence <0.2 to very high coherence >0.9 [9].
3. Statistical analysis
A descriptive analysis of the data was conducted regarding the achievement of medical competence and professional behavior among medical graduates. Using IBM SPSS ver. 24.0 (IBM Corp., Armonk, USA), we captured the demographic data of participants and analyzed it. AMOS ver. 26.0 (IBM Corp.) was used for structural equation modeling of the six latent variables and 35 indicator variables, which yielded a structural equation showing the five most favored domains related to the management of patient ability.
The coefficient-Cronbach’s α value was used to assess the reproducibility of the questionnaire [10]. According to Guilford [11], the level of internal consistency can be classified into five categories: very low reliability (r11 <0.2), low reliability (0.2< r11 <0.4), moderate reliability (0.4< r11 ≤0.7), high reliability (0.7< r11 ≤0.9), and very high reliability (0.9< r11 ≤1.0) [11]. A Cronbach’s α value (r11) of more than 0.7, therefore, indicated that a high internal consistency had been achieved [12,13]. The 35-item questionnaire had a very high coherence as evidenced by Cronbach’s α of 0.916 and each domain has Cronbach’s α as follows: professional behavior value of 0.875; humanism value of 0.849; clinical skill competence value of 0.814; patient management value of 0.832; interpersonal skill value of 0.785; and cognitive competence value of 0.624.
The potential for bias when completing the questionnaire due to respondents’ fear of their honest feedback affecting lecturers’ performance assessments was recognized. To address this, the researcher ensured that participation in this study was voluntary and that their evaluation would have no implication for the lecturer.
4. Ethical approval
Ethical clearance was obtained from the Research Ethics Committee of Al Ihsan Hospital (no., 70/4086/KEPK-RSUD Al Ihsan/2022). The ethical aspects of this study include respect for a person by asking for approval after explanation, the confidentiality of the identity information of the research subject/medical graduates, justice, and not causing harm to the research subject. All the participants in this study have given consent and agreed to participate, allowing the data to be analyzed and published in a scientific journal.
Results
The demographic characteristics of participants on 206 medical graduates were based on gender, age, batch, and length of time from graduation. We captured the demographic characteristic as seen in Table 1. Based on Table 1, it was found that the female graduates are greater than male graduates with a ratio of 3:2. The length of time since graduates were dominated by alumni that have graduated 2–5 years and were followed by 6–9 years, and the last >9 years.
The medical graduates’ employment distribution is given in Table 1, which shows in descending order, that participants were employed as follows: other (i.e., private medical practice, corporate, and so forth), public hospital, private hospital, degree-granting school, primary health care center, and college, as a lecturer.
Of the 206 medical school graduates, they have a very good perception of humanism—the character of good doctors’ concern with holding religious values (score of 68.98%–95.67%) and interpersonal skills (score of 18.80%– 91.26%). Based on Table 2, the aspect of clinical skill competence was rated the smallest by medical graduates. This is due to the ability of clinical skills to continue to develop in line with the advancement of medical science and technology. Thus, doctors should be willing to update their medical knowledge and clinical skills.
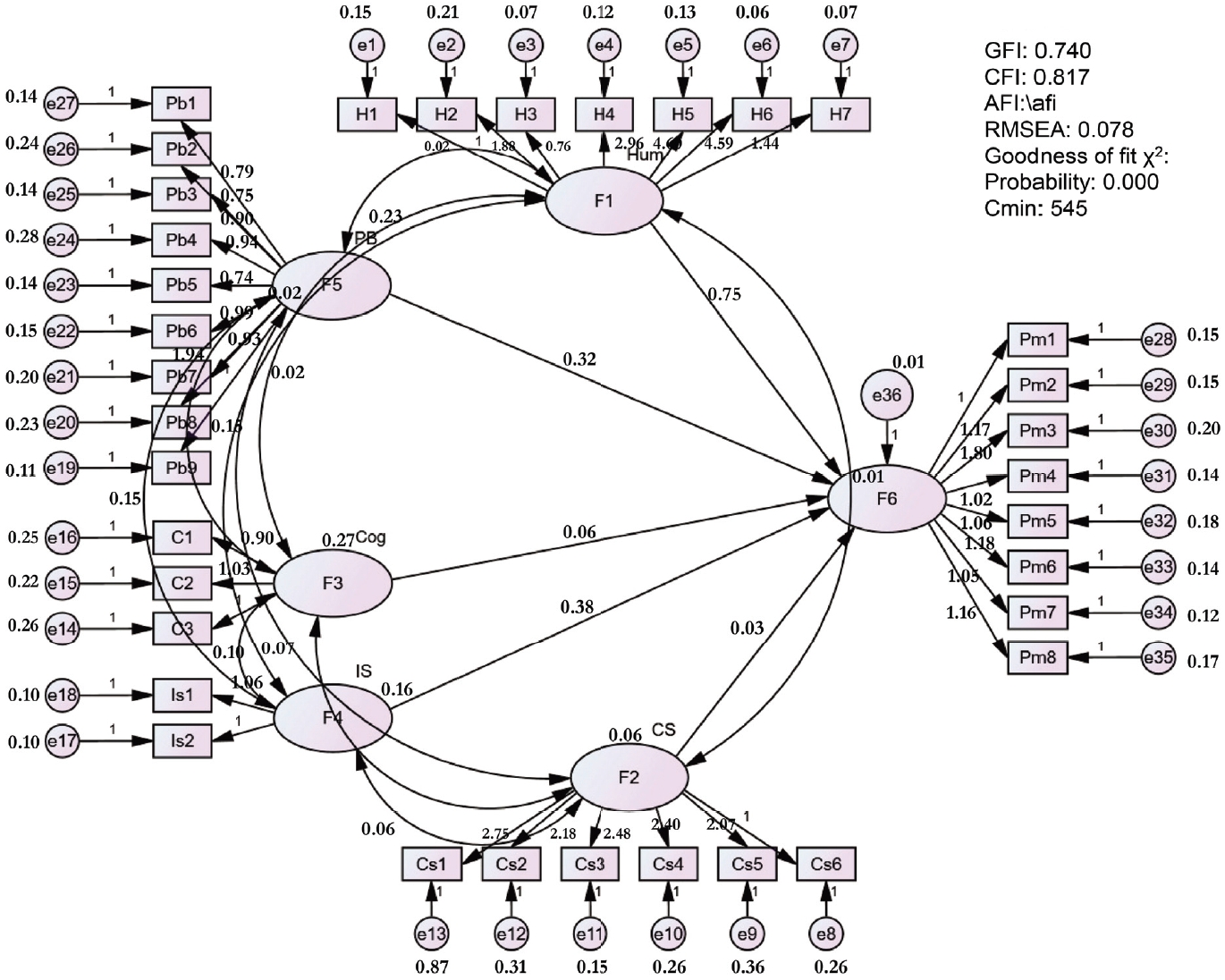
A model of structural equations for the factors that influence the management ability of patients is shown in Fig. 1. Fig. 1 depicts that the domain of professional behavior, humanism, interpersonal skill, clinical skill, and cognitive competence contribute to the patient management ability of graduates. A structural equation model of various factors affecting patient management ability is acceptable because it meets the following estimated parameters: root mean square error of approximation (RMSEA) value <0.08 (0.078: good fit), the value of chisquare minimum/degree of freedom (CMIN/DF) >2 and less than 3 (2.241: good fit), and comparative fit index (CFI) >0.9 (0.817: marginal fit) [13].
The magnitude of the influence of each factor/domain on the ability to manage patients shows how much these factors contribute to affecting a determining factor (patient management). The model and influence of each factor are shown in Table 2. Based on Table 2, our study showed that factors of humanism, professional behavior, and skill of interpersonal influence the managing ability of patient significantly with p-value as follow: 0.035, 0.000, and 0.00, respectively as well as critical rate value >1.96. While two other domains (clinical skills competence [p=0.731] and cognitive competence [p=0.2]) have no significant effect. This is likely due to these two factors being components that must be mastered before graduating as a doctor.
The relationship between factors and some of their indicators can be seen in Table 3. This table illustrates that all indicator variables significantly represent each of their latent variables. This is indicated by all critical rate values of items having a value of more than 1.96. Based on Table 3, our finding also depicted that the humanism domain (F1) is most favored by item H6 (critical rate value=2.911; showing politeness and respect to the patient and his family). Professional behavior (F5) is most represented by item Pb6 (good problem solver) and it has a critical rate value of 12.748. The interpersonal skills domain is most favored by item Is1 (ability in the team-working) with the critical rate value is 11.129. While item c2 (case variation during the clerkship) significantly represents the cognitive competence aspect with a critical rate value of 8.509. Item Cs3 (skilled in handling patients with trauma) is the most represented clinical skill ability aspect, and it has a critical rate value of 5.801.
Discussion
The main objective of the study was to identify the most influential factor in the achievement of medical competence toward patient management ability. There are three components that were deemed important and have achieved excellent aspects in terms of humanism—the character of good doctors’ concern with holding religious values, interpersonal skills, and professional behavior.
Humanism refers to the qualities of being a human that relates to physician roles and is based on Islamic values as a benchmark for the character of good doctors’ concern with holding religious value [14,15]. Both aspects of professional behavior and humanity are part of the development of the professionalism of a medical doctor. At the same time, interpersonal skill emphasizes subordinate communication, cooperation, peer communication, community perspective, personal instinct, the opportunity for improvement, and self-confidence. In line with the objective of this study, our work indicated that humanism, interpersonal skill, and professional behavior are three aspects that dominate in assessing the ability of patient management. It is undeniable that in the patient-doctor relationship, aspects related to human nature, well-being, and behavior shown in the order of professionalism of the doctor become crucial factors for achieving the goals of treatment. Clinical competence refers to a number of abilities and skills a physician must be mastered to practice medicine. A doctor’s clinical competence has three important aspects: sufficient medical knowledge, skills, and practical behavior in terms of judgment and experience for express purposes [16]. Webster’s Dictionary defines being competent as the quality of having sufficient knowledge, judgment, skill, or experience for a particular purpose. It could be reasoned that diagnosing illnesses and providing interventions to improve the patients’ condition are among a doctor’s primary duties [6,17].
1. Comparison with previous studies
Conran et al. [17] found that the development of medical professionalism should start in an early medicine program. Trainees entering graduate medical education should have already developed professional behavior. This is learned behavior; hence, professional behavior is modifiable [17]. Regarding medical competency, faculty management should consider certain factors. This is in line with the findings of the present study, which advises that a medical education program will be very helpful in building a professional identity. Professionalism must be taught early, longitudinally, and deliberately using both targeted instruction and experiential learning.
Regarding professional behavior, our finding is in accordance with the study by Reynolds et al. [18], which involved 365 residents as research subjects. They found that residents perceived their commitment to professionalism to be greater than that to the institution where they work. Furthermore, Forouzadeh et al. [19] concluded that the development and strengthening of professionalism are correlated with the establishment of a desired professional identity. The humanism domain in the present study (subscale 6: showing politeness and respect to the patient) is in line with the review by Macneill et al. [20] conducted in Singapore. They found that respect is one aspect of humility in addition to compassion, integrity, and empathy when developing medical professionalism. Similar to the concept of medical professionalism in Arabic and Chinese frameworks, our study indicates that religiosity and moral values are the most important subscale of an area of concern [21].
Regarding medical competency in terms of cognitive competence, clinical skills, and interpersonal skills, our result differed slightly from the study by Ahmadipour and Mozafari [22] in Iran involving 57 physician graduates. The most important aspect of patient management according to those scholars relates to the ability to evaluate patient history, and undertake physical examination and diagnostics, whilst our work indicated the significance of psychological support to help patients recover faster, in addition to discipline and improvement of medical sciences. Clinical skills deemed important to our graduates were handling trauma and burn injuries. Ahmadipour and Mozafari [22] found that suturing and measuring hematocrit are regarded as essential procedural skills in Iran.
2. Limitations
There was a low risk of selection and performance bias. We used stratified proportionate random sampling to choose each graduation batch participant. We collected data using a validated instrument, and the member team was unaware of whether the participant judged earnestly and honestly or not, even if, in the approval of the study, the researcher asked for the participant to answer truthfully.
3. Conclusion
Structural equation modeling of several factors influencing patient management ability highlighted humanism —good doctors’ concern with holding religious value, professional behavior, and interpersonal skills as factors that significantly contributes to their patient management ability. Primarily, the model is acceptable because it meets the parametric criteria as follows: RMSEA <0.08 (0.078), 2< CMIN/DF <3 (2.241), and the CFI closely approaches 0.9 (0.817).
Further research is needed to compare patient management ability at other institutions and in other countries. It is also necessary to conduct research including all alumni of the UNISBA Faculty of Medicine.