Introduction
Longitudinal integrated clerkships (LICs) have been introduced in various medical schools and come in a variety of forms [1,2]. A review of LIC research published between 1996 and 2012 demonstrated that students in LICs achieved equivalent or better academic results compared to traditional rotation-based clerkship students on knowledge and clinical skills examinations [3]. LIC students were found to be more satisfied than traditional clerkship students with their learning [4], felt better prepared to deal with ethical dilemmas [5], and expressed the educational value of the clerkship program in terms of mentoring [6]. Three common elements of LICs are participating in the comprehensive care of patients over time, maintaining learning relationships with these patients’ clinicians, and meeting the majority of the academic year’s core clinical competencies across multiple disciplines [2]. However, most previous research compared LICs with traditional clerkships, so little is known regarding which elements of LICs are responsible for the differences from traditional clerkships. Most research on LICs is related to the development of the curriculum, whereas there is little research on the factors necessary to maintain a sustainable LIC program [7].
Learning relationships with clinical faculties, junior hospital doctors, or peers is an important factor in medical education. Many studies have found that relationships with faculty members helped students receive the feedback and assessment needed for the development of expertise [8,9]. Interactions between faculties and students in traditional clerkships enhance the learning of undergraduate medical students [10]. Furthermore, this effect in clerkship has been studied in the context of team-based learning and resident training [11,12]. Medical students in LICs are paired with a clinical faculty member for the duration of an extended period, whereas rotation-based clerkship students are usually supervised by multiple clinical faculty members for relatively short periods. However, both traditional clerkships and LICs face challenges in promoting continuing relationships between students and the patients’ clinicians. In a block rotation clerkship, students’ learning relationships with faculty members were mainly governed by impression management, and students were not regularly coached by faculties on diagnostic thinking [13]. Feedback through relationships is key to advancing to the highest level of teaching and learning. It may be provided formally through a structured supervisory relationship or informally through learning relationships with peers [14,15]. Nonetheless, teaching in the clinical environment is a demanding, complex, and often frustrating task. To overcome this limitation of feedback, portfolios have also been used in the field of medical education [16].
In 2018, Seoul National University College of Medicine introduced a patient-centered LIC program in combination with a traditional clerkship. The main outcomes of our program are to understand the continuity of care and the concept of patient-centered care. The patient-centered LIC program lies between the amalgamative clerkship and the blended LIC, according to the typology of LICs [1]. However, our LIC program is not complemented by the block-rotation clerkship; instead, the block-rotation clerkship is complemented by the LIC. We aimed to complement patient-centered care, and, therefore referred to our program as a “patient-centered LIC.” Our model is a parallel streaming model with specific preceptors. The program was conducted in the penultimate year with a 1-year clerkship length. All third-year students participated in the LIC program, which was a mandatory course. The two main characteristics of our LIC are regular discussion classes and an e-portfolio. We hold discussion classes to strengthen student-faculty and student-student interactions. During all discussion sessions, we matched one faculty member per discussion group to form relationships with students. Each student’s assessment was determined by the group report, peer review, attendance, and final report for each session. Early results of the first 2 years of this program were presented in the previous article [17].
The purpose of this study was to investigate the characteristics of student-faculty and student-student interactions in the LIC program and to identify other factors related to whether students understood and acquired the program’s main outcomes.
Methods
1. Study design and paricipants
The study was conducted among the 149 third-year students at Seoul National University who participated in the LIC program in 2019. Before the semester began, we recruited participating clinical faculty members and held a meeting of the LIC committee. At the beginning of the LIC program, we presented students with an overall overview of the program, including the concept of patient-centered care, the concept of continuity of care, and the procedures of the small-group discussion classes. Classes on the concepts of the continuity of care and patient-centered care were also included in the preclinical curriculum. Each participating clinical faculty member provided the office of medical education with a list of hospitalized patients suitable for long-term follow-up. Two patients were allocated to a pair of students sharing the responsibilities, and long-term follow-up began. The students met patients when patients visited the hospital, and if doing so was not possible, students followed up their patients by reviewing the patients’ electronic medical records. Depending on the patient’s schedule, students followed up their patients for at least 6 to 9 months. Patient allocation was carried out for 1–2 months, and the discussion classes began when all students had been assigned a patient. The topics of discussion classes were the patient-physician relationship, clinical decision-making, medical ethics, team care, end-of-life-palliative care, and patient-centered care. Before and after the discussion classes, clinical faculty members and facilitators met to debrief and share feedback on each class. Students conducted discussion sessions, under the supervision of faculty members conducted discussion sessions with larger classes. Students received feedback from the clinical faculty member, and feedback was provided during the discussion class and through an e-portfolio. Clinical faculty members and students were matched through an e-portfolio system, where records were approved and feedback was given. Students wrote initial assessment notes, progress notes, and final reports in the e-portfolio (Fig. 1). We divided the students into groups of eight for small-group discussions. These groups were organized into corresponding discussion classes, which were held 7 times a year, with one facilitator and/or one clinical faculty member in each class, according to a set topic. There were four class sections, each of which consisted of 32 to 40 students (i.e., four to five groups of eight) for inter-group discussions. The clinical faculty members involved consisted of a total of 29 faculty members from six departments: internal medicine, general surgery, obstetrics and gynaecology, paediatrics, orthopaedic surgery, and neurology. During the discussion classes, students had discussions with clinical faculty members and peers and received feedback. In total, 150 patients were enrolled in the program.
The course evaluation questionnaire was completed by third-year medical students (Appendix 1). The questionnaire included 22 items measured on a 5-point Likert scale and covering three domains: student experience, discussion classes, and self-assessment. After a frequency analysis of responses to the items was conducted, logistic regression analysis was carried out to identify associations with positive learning experiences. The main purpose of this study was to investigate the characteristics of student-faculty and student-student interactions in the LIC and to identify other factors related to whether students understood and acquired the program’s main outcomes. Additionally, we tried to identify other factors related to whether students understood and acquired each topic of the discussion class.
2. Statistical analysis
To assess factors associated with the self-estimated educational effect by students, 5-point Likert-scaled responses of outcome variables were analysed as dichotomous (strongly agree/agree versus neutral/disagree/strongly disagree). We compared variables related to students’ experiences and discussion classes according to whether students answered that the LIC was more helpful than traditional clerkships using binary logistic regression with stepwise backward elimination based on the likelihood ratio. We retained associated factors with a p-value less than 0.10 for the multivariable analysis to determine the explanatory contribution of those variables in terms of students’ self-estimated understanding and acquiring each outcome of the program. All analyses were conducted using the IBM SPSS statistical package ver. 26.0 (IBM Corp., Armonk, USA).
3. Ethics statement
The Institutional Review Board of Seoul National University College of Medicine and Seoul National University Hospital exempted this study from review since it was an analysis of de-identified data (E-2001-016-1091). The requirement for informed consent from individual participants was omitted.
Results
In 2019, 149 students participated in the LIC program, 144 of whom returned valid questionnaires. In terms of student-faculty interaction through e-portfolios, 12 students on average were assigned per clinical faculty member, with 332 admission notes, 1,409 progress notes, and 303 final reports, and an average feedback time of 32 days. Of the 2,044 total records, 1,988 records (97.3%) were approved and feedback was received from clinical faculty members.
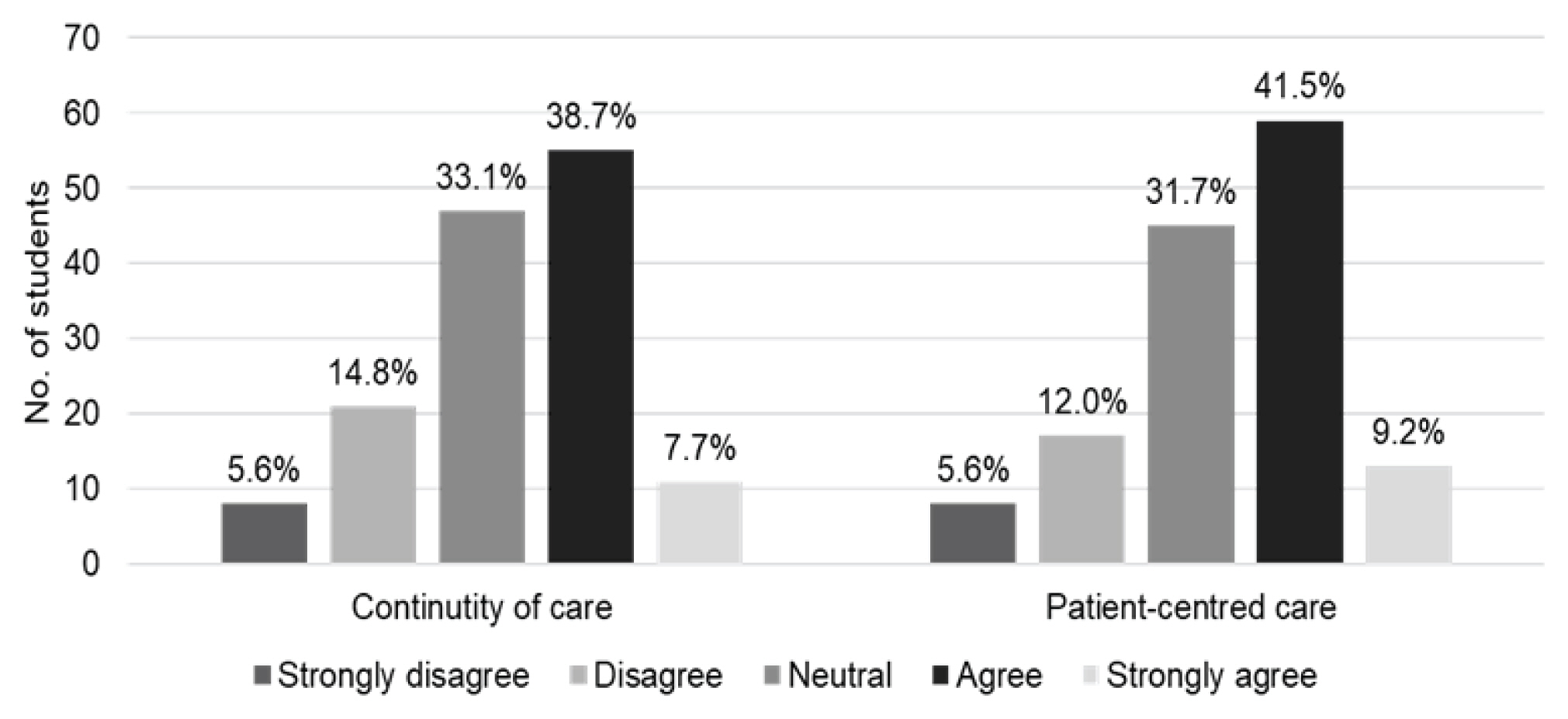
The distribution of students’ responses to the questionnaire about the main outcomes is shown in Fig. 2. Logistic regression analysis was used to identify associated factors and to adjust for confounding factors. Relevant feedback from faculty members in discussion classes (adjusted odds ratio [AOR], 5.071; p<0.001), motivation by e-portfolio feedback (AOR, 1.790; p=0.026), and frequency of e-portfolio feedback (AOR, 1.813; p=0.012) predicted a greater likelihood of understanding the continuity of the patient’s medical experience (Table 1). Relevant feedback from faculty members in discussion classes (AOR, 3.445; p<0.001) and frequency of e-portfolio feedback (AOR, 2.232; p<0.001) also predicted a greater likelihood of understanding the concept of patient-centered care (Table 2).
For understanding and acquiring the outcomes related to each discussion topic, binary logistic regression showed that the following factors had independent relationships with the outcome variables: relevant feedback from faculty members in the discussion class, frequency of received e-portfolio feedback, motivation by e-portfolio feedback, and the activeness of discussions between groups. However, differences were found in the specific factors across the various topics (Table 3). For student-student relationships, the activeness of discussions between groups was positively associated with understanding the concept of the patient-physician relationship (AOR, 4.710; p<0.001), whereas cooperation with the paired student was negatively associated with this outcome variable (AOR, 0.529; p<0.033). The adequacy of the assigned patients was negatively associated with understanding the concept of palliative care (AOR, 0.547; p<0.043).
Discussion
This study documented the effects of student-faculty interactions and student-student interactions in a LIC program and identified other factors related to whether students understood and acquired the main outcomes of the program. Feedback in discussion classes and frequency of e-portfolio feedback were important factors for obtaining outcomes in our LIC program. Strengthening learning interactions through discussion classes and an e-portfolio had a positive effect on the LIC program.
Student-teacher relationships are an important element of education in clinical clerkships. However, the traditional rotation-based clerkship has limitations in making reliable judgments or allowing meaningful participation because the relationship between students and clinical faculty members is fragmented [18]. Several factors contribute to this unfavourable educational environment including limited time, patients avoiding clerkship education, shortened patient hospital stays, and lack of continuity of patient care after discharge [19]. To overcome this environment, LIC programs are being introduced by increasingly many medical schools as an alternative to traditional clerkships. The LIC educational structure relies on developing a complex “panel” or “cohort” of patients [1]. In our study, two patients were allocated to a pair of students, and groups of eight students shared experiences with eight patients. Because each discussion class consisted of four to five groups, the total panel of patients discussed comprised 32 to 40 patients. The relatively small number of patient panels and few chances to meet clinical faculty members due to the parallel rotational clerkship were limitations of our program. To compensate for this, we used group discussion classes to share more patient experiences and to continue learning relationships with these patients’ clinical faculty members. Another strategy to enhance faculty-student interactions was the use of an e-portfolio system. Portfolios are used in education to help students reflect on their academic goals, to determine whether students have met academic requirements, and as a basis for teachers to provide feedback helping students to grow, improve, and mature as learners [20]. Portfolios are used in various fields of medical education [16], and can be utilized to collect evidence of performance and reflections on the clerkship to document learners’ personal and professional development [2]. In graduate medical education, portfolios are effective and practical in several ways, including increasing personal responsibility for learning and supporting professional development [21]. The format of portfolios can be primarily paper-based or electronic. Research has shown that electronic portfolios have several advantages over paper-based portfolios [22]. According to the results of this study, both strategies seemed to play an important role.
In the analysis related to the primary purpose, no significant results were found for student-student relationships, but the analysis related to each discussion topic showed statistically significant results associated with student-student relationships. The group discussion class not only strengthened faculty-student relationships, but also had the effect of collaborative learning by facilitating interactions between students. Collaborative learning partnerships between peers can increase productivity and help students to develop specific skills [23,24]. The effects of these collaborations in small-group classes–as exemplified by student-faculty interactions and student-student interactions in team-based learning in LIC programs–are well known [11,25]. An appropriate role of the teacher can facilitate and encourage these collaborations. Learning partnerships between peers in LICs are not well-understood. In our study, we were able to see some independent associations, such as active inter-group discussions and collaboration with co-students. However, in the context of the patient-physician relationship, collaboration with co-students showed negative effects. This result might be associated with free-riding and social loafing on collaborative tasks [26]. We tried to prevent these shortcomings and facilitate discussion by conducting peer evaluations within a single group of eight students. However, the way we assigned two patients to two students had both positive and negative aspects. For example, in some cases, both students in a pair submitted the same progress note in the e-portfolio, although each student was required to do so separately. Improvements will be needed for peer assessment at the student-pair level or in intergroup discussions.
Assigning appropriate patients is an important part of the LIC program, and it was somewhat difficult to interpret whether this component of the program was successful in this study. Although some assigned patients did not provide an adequate basis for the discussion of each topic, students were nevertheless satisfied. However, for palliative care, the adequacy of the assigned patient was assessed negatively. Although each discussion class is, in principle, based on a patient assigned as part of the LIC, the discussion class on the topic of palliative care was based on a more appropriate patient experienced in the rotational clerkship if the assigned patient was not appropriate. This might have caused the negative associations. In brief, it is speculated that students who were not assigned appropriate patients gave positive responses regarding the helpfulness of the rotation-based clerkship because patients from that clerkship served as the basis for discussions.
The present study has some limitations. First, our results demonstrated only associations, not causality, since this was not a case-control study. In addition, factors particularly related to student-student relationshisp, which constituted one of the purposes of the study, were not identified as relevant to the main outcome of our LIC program. Third, the explanations of some negative associations were not conclusive, although we suggested some possible explanations. However, these limitations give further insights into the organization of groups, classes, and the program, which could be the subject of further research in the future. The unique characteristics of our LIC program are also a limitation. Caution should be taken in interpreting the results and applying them to other LICs. Our program partially shared the characteristics of both amalgamative clerkships and blended LICs. It is a mandatory course covering the majority of disciplines that complements the block-rotation clerkship. Our LIC had relatively few sessions, but we tried to complement the continuity of relationships through an e-portfolio.
In conclusion, student-faculty interactions were found to be important factors in the LIC program. Group discussion classes and the use of an e-portfolio could be effective tools to enhance learning in a patient-centered LIC. Relevant feedback from faculty members in discussion classes, motivation by e-portfolio feedback, and frequency of e-portfolio feedback were independent factors for understanding the main outcomes of the course. Student-student interactions, such as active student-to-student discussions and the progress of appropriate student discussions, were found to be associated factors. It is still not clear the degree to which improved feedback enhances students’ learning in LICs; however, we provided more evidence that there is an important unresolved issue. Further research will be needed on educational effects and mechanisms to enhance students’ learning in LIC programs.