Nurikhwan, Felaza, and Soemantri: Burnout and quality of life of medical residents: a mixed-method study
Abstract
Purpose
Currently there are a limited number of comprehensive studies exploring in more depth the relationship between burnout and quality of life (QoL) of medical residents during residency training. This study aims to examine the correlation between burnout and residents’ QoL and explore the factors associated with burnout in residency training.
Methods
This was a mixed-method study. The first stage was a quantitative study using cross-sectional design to administer the Maslach Burnout Inventory Human Service Survey and World Health Organization Quality of Life-BREF instruments to 86 medical residents, followed with the qualitative study through 10 in-depth interviews.
Results
Twenty-seven residents (31.4%) experienced severe emotional exhaustion (EE), 22 (25.6%) experienced severe depersonalization (DP), and 40 (46,5%) experienced low personal accomplishment (PA). Factors increasing the likelihood of experiencing burnout were being surgical residents for EE (2.65 times), dealing with difficult/rare cases for DP (1.14 points), and working hours for PA (1.03 points). The QoL was influenced by the three burnout domains, marital status, education level, gender, age, type of residency, night shift, difficult/rare cases, working hours, and number of emergency cases. Factors influencing burnout, both intrinsic and extrinsic, were identified and divided into causative and protective factors.
Conclusion
The current study has examined the relationship between burnout and QoL and identified factors affecting residents’ burnout. Both intrinsic factors, such as spirituality, and extrinsic factors which include duration of shift, work facilities, and teacher-senior-junior relationships, affect burnout. Supervision and academic regulation are some of the solutions expected by the residents to minimize burnout.
Keywords: Burnout, Quality of life, Internship and residency
Introduction
Burnout is a state describing a response to chronic work-related stress, and consists of three dimensions, emotional exhaustion (EE), depersonalization (DP), and decreased perceptions of personal accomplishment (PA) [ 1, 2]. This state was discovered to be at a higher rate among medical residents (39% to 85%) compared to medical students (28% to 45%) [ 3, 4]. The factors influencing burnout are classified as either intrinsic, comprising demographic characteristics (gender and age), social conditions, psychological conditions, and individual characteristics, or extrinsic, including work environment and organizational factors [ 5]. Residency program is a postgraduate medical education and an in-depth mastery training of certain field (specialty) of medical specialties, with independent learning methods as well as supervision. Residents undergo learning processes in teaching hospitals through providing specialized health services to patients, and this often causes significant stress levels, resulting in burnout. Residents with burnout tend to experience barriers while working, personal health and well-being deterioration, obstacles in building social relationships, difficulties in determining diagnoses (diagnostic dilemma), as well as experiencing difficulties in their ability to provide optimal patient care and to perform academically [ 1]. Quality of life (QoL) is a multidimensional standard level consisting of individual or community expectations for a good life [ 6]. A decrease in life quality tends to occur in residents with burnout, and this possibly leads to depression, risk of medical errors, and jeopardizes patient safety through misdiagnosis and errors in therapy [ 1]. The Maslach Burnout Inventory (MBI) remains a suitable instrument for measuring burnout. Based on the meta-analysis results, MBI has high reliability in all three domains, high test-retest reliability, and the ability to assess community service-related works. This instrument also has several variations depending on their context of which they were utilized. MBI focusing on assessing work in community services is called the Maslach Burnout Inventory Human Service Survey (MBI-HSS) [ 7]. The instruments to measure QoL can be divided into general and specific instruments. General instruments are used to measure the QoL in general, including functional abilities, disabilities, as well as concern about getting sick. Some of the most frequently used instruments include the World Health Organization Quality of Life (WHOQOL)-BREF, Short Form-36, and EuroQOL-5 Dimension [ 6]. Meanwhile, specific instruments are used to measure specific aspects of disease (e.g., QoL Questionnaire in Schizophrenia), certain populations (e.g., in the elderly), or special functions (e.g., emotional functions) [ 8]. Currently, studies exploring the measurement of QoL and its relationship with burnout among residents is very limited [ 9- 11], and has not been linked to other factors, such as length of working experience, phase of study, and number of cases encountered. This study therefore aims to examine this relationship and explore the factors associated with burnout in residency training. The findings from this study are expected to serve as a basis for formulating burnout prevention and management program in residency program.
Methods
1. Study context
The study was conducted in six residency programs of one public medical school in Indonesia from January to July 2020. Residency program in Indonesia is university-based. The length of study varies depending on each residency field, but in average it takes 7–11 semesters to complete the program. As doctors in training, residents are assigned with certain clinical responsibilities either in outpatient or inpatient settings, under consultant supervision, according to their phase of study. Residents must pay tuition fee each semester and clinical teaching and learning process is conducted by a team of clinical teachers from each department. The rights and obligations of residents are determined together by the faculty of medicine and teaching hospital.
2. Study design
This study used a mixed-method design carried out in two stages to obtain comprehensive understanding of burnout in residency program. The first was a quantitative study, with a cross-sectional design, using the MBI-HSS and WHOQOL-BREF instruments, to identify the level of burnout and QoL of residents. Qualitative design was used in the second stage through in-depth interviews to explore the factors associated with residents’ burnout.
3. Study participants
Six residency programs were selected based on the representation of surgical (surgery, obstetric and gynecology, anaesthesiology) and non-surgical disciplines (internal medicine, pulmonology, paediatric). These six programs have also represented the larger department in the hospital (surgery, obstetric and gynecology, internal medicine, and paediatric) and the smaller ones (anaesthesiology and pulmonology). The study participants for the first stage were 86 medical residents from six residency programs of one public medical school in Indonesia. The number of sample was deemed sufficient based on the sample calculation formula for cross sectional study [ 12]. In stage two, 10 resident participants were purposively selected using a maximum variation sampling strategy by sampling participants from each group of gender (male/female), marital status (married/not married), phase of study (semester 1–2/semester 3 and above), and burnout level (low, moderate, high). This purposive sampling was intended to obtain complete perspectives regarding factors associated with burnout from respondents with different background.
4. Data collection
Data collection in the first stage was conducted using two online questionnaires, MBI-HSS and WHOQOL-BREF. In addition to that, participants’ demographic data were also obtained, such as age, gender, type of residency program and marital status, the number of working hour and night shifts per week, number of emergency/death cases, and difficult/rare cases per week ( Table 1). Meanwhile, in the second stage, data collection was carried out through in-depth interviews conducted by the researcher, guided by open and probing questions developed based on key literature about the burnout causes. The interviews were audio-recorded. All participants provided their consent upon their involvement in the study.
5. Data analysis
Descriptive analysis using IBM SPSS ver. 23.0 (IBM Corp., Armonk, USA) was applied to the data of gender, type of residency program, marital status, phase of study, the number of working hour/night shifts, and the number of death and difficult cases. Burnout score and WHOQOL-BREF scores were also calculated. The burnout scores were distributed into the three subscales (domains) within the MBI-HSS, which were EE, DP, and PA. Each item in the subscale was measured using a 7-point Likert scale and the scores of the subscales were grouped based on the cut-off score for each category of low, moderate, and severe/high according to Maslach et al. [ 7]. A multivariate analysis using linear regression test (for QoL variable) and logistic regression test (for burnout variable) was also carried out to examine the relationship between the demographic variable with burnout and QoL. Verbatim transcriptions were made based on the interview recordings. A thematic analysis was conducted manually by all authors. The first author read the first two transcripts and identified relevant themes and subthemes. A coding system was developed and agreed by all authors. Subsequent analysis of the remaining transcripts followed the coding system and any new themes and subthemes were added. Data display and conclusions drawing and verification, including member checking, followed the process [ 13].
6. Ethical clearance
This study received ethical clearance from the Universitas Lambung Mangkurat (No.060/KEPK-FKUNLAM/EC/II/2020).
Results
1. Results of MBI-HSS and WHOQOL-BREF survey
Eighty-six residents completed the surveys. The MBI-HSS scores were divided into three levels (low, moderate, and severe/high) based on the categorization from Maslach et al. [ 7]. The mean score of each domain of QoL was calculated with the possible range of QoL score of 0–100 for each domain. The score distribution of both MBI-HSS and WHOQOL-BREF is provided in Table 1. The results of the linear and logistic regression were presented in Table 2. The variables affecting EE were surgical residency program and QoL domain 2. Based on the results, the surgical residents had a 2.65 times higher tendency to experience EE, compared to the non-surgical residents. In terms of the QoL each unit in the domain 2 increased the EE score by 0.91 points. Meanwhile, for DP, handling difficult/rare cases increased the DP score by 1.14 and any decrease in working hours increased the PA score by 1.03 points. The table also shows an equation model for each QoL domain. For example, every increment in residents’ age, increased physical domain by 0.813 point, decreased psychological domain by 0.29 point, increased social domain by 0.30 point and increased environment domain by 0.10 point. The rest of the equation models for all domains were available in Table 2.
2. In-depth interviews analysis
Table 3 shows the characteristics of 10 residents involved in the in-depth interviews. Based on the thematic analysis, intrinsic and extrinsic factors influencing burnout were identified. Each of these factors was further divided into burnout causative and protective factors ( Fig. 1). The burnout impact and the institutional support system in protecting burnout among residents were also identified.
3. Burnout intrinsic factor
Burnout causative factors are factors within the individuals that influence the occurrence of burnout. Several of these factors identified in this study include physical exhaustion, personality, motivational and time management, as described below by some of the participants.
“Physical fatigue is caused by the work schedule, the number of patients, the severity of the patients, hence with such a load, they may experience burnout quickly.” (respondent [RESP]-9) “Honestly, personally, I feel that I am a perfectionist. … it is one of the reasons that causes pressure other than the outside environment, especially for myself, who is sometimes too demanding [to myself], too perfect.” (RESP-7) “In my opinion, what can cause the burnout, first, is [when we have] a field of interest that is not in accordance with the program [that we are in now] or do not match reality.” (RESP-9)
Meanwhile, the protective factors can prevent burnout from within the individual. Based on the in-depth interviews, these factors include personality, coping stress, adequate rest, and spirituality.
“We have to be open minded, if we are closed minded, whatever our problems are, it is hard to solve [them], if we are open, there are many ways, whatever the problem is.” (RESP-10)
Some respondents mentioned refreshing activities as the way to protect oneself from burnout.
“Furthermore, to reduce burnout, maybe I start with activities that can make me happier, for example, if I have free time, maybe I can take up more hobbies, such as futsal, running, and cycling. I don’t just focus on academic activities so that it prevents me from doing other activities.” (RESP-9)
Respondents also mentioned that spirituality helps in overcoming problems during study.
“Because we are Muslims, first of all, to be honest, during the demanding clinical rotation, it felt like I was much more obedient [to God], perhaps out of fear, so I did more worshipping and also prayed more diligently.” (RESP-7)
4. Burnout extrinsic factor
Extrinsic factors causing burnout are workload, working system, hierarchical working relationships (with attending physician and senior residents), limited number of residents, and also inadequate supporting facilities/equipment. According to the participants, there are difficulties in keeping with the working schedule and system of the residency program. Long working hours is also a factor mentioned by the residents.
“In my opinion, overworked contributes to residents burnout, … working in the shift all day long and continued with another shift in the next day. In some rotation, the shift finished at 7 PM or 10 PM.” (RESP-4) “In the first semester, the difficulty was in following the initial rhythm of the residency [program].” (RESP-5) “The changes in the system due to a shortage of residents caused our shift to be extended, originally [finished at] eight [now] became 10. At first, we were only supposed to stand by at the ward, now we had to also stand by at the emergency room.” (RESP-1) “Limited materials when treating wounds, such as the unavailability of gauze, has made us run again to a place providing it. This is also a factor of burnout.” (RESP-6)
The external factors protecting burnout include support from peer and family and also the institutional support system.
“To prevent burnout, we can ask friends for help because the surgery program teaches teamwork. We have made a commitment to help other friends if there is a problem.” (RESP-6) “In obstetric gynecology department, there is a team, if someone is having burnout, his/her friend or senior automatically has to back him up. We were very trained from the first semester to be able to cope and solve problems.” (RESP-3)
5. Negative effects of burnout
Burnout had negative impacts on both the physical and psychological state of the residents and also their work and academic performance. Some residents mentioned the lack of focus which often caused self-endangering. Meanwhile, performance-related impacts include suboptimal healthcare service, missed schedules and academic targets, and increased dropout rate.
“Resident burnout is dangerous. For example, lack of focus during injection administration may cause harm, or when he comes home from work with unfocused and conscious mind, may prone to accidents.” (RESP-2) “The common health problem during burnout is to become sick more often. Burnout may even create self-harming thoughts such as injuring yourself or having thoughts of suicide.” (RESP-9)
6. Strategies to minimize burnout
According to the study participants, the institutional support system is the factor expected to prevent or minimize burnout. The institutional support system includes academic regulation, supervision, psychological support, burnout screening, and leisure activities. Some respondents mentioned the need for the institution to regulate the residents’ working hour.
“There needs to be a standard [of working hour] that was set by policymakers. For example, it is necessary to follow the work schedule for a week, not exceeding the predetermined number of hours.” (RESP-9)
Institutions ought to facilitate interaction between senior and junior through leisure activities, such as sports, to make communication more relaxed. The study program ought to also allocate more time to listen to the residents’ problems and create solutions.
The participants also expect the institution to provide professional psychological support provided by psychologists for the problems experienced by the residents.
Some participants suggested that screening for a tendency to experience burnout at the time of admission is required on a regular basis.
7. Summary of findings
Fig. 2 summarized the study findings and the relationship between those of the quantitative and qualitative stage. The variables affecting EE were surgical residency program and QoL domain 2. Surgical residents had a 2.65 times higher tendency to experience EE, compared to non-surgical residents. For the QoL domain 2, each unit increased the EE score by 0.91 points. Residents handling difficult/rare cases increased the DP score by 1.14 points, compared to residents without difficult/rare cases. Meanwhile, every drop in the number of working hours increased the PA score by 1.03 points.
The QoL variable has four domains, 1 (physical health), 2 (psychological), 3 (social relationships), and 4 (environment). The study demonstrated that each QoL domain was influenced by one to three burnout domains, marital status, phase of study, gender, age, type of residency program, night shift, difficult/rare cases, duration of working hours, and number of emergency cases.
Two factors were identified to influence burnout experienced by residents, namely burnout intrinsic and extrinsic factors, which can be either causative or protective of burnout. The negative impact of burnout and the institutional support system expected to protect residents from burnout have also been elaborated.
Discussion
This study demonstrated burnout incidents in residency program in one teaching hospital in Indonesia in which 32.6% residents had a high level of burnout in at least one aspect of PA, DP, or EE. These results are in line with the study by Zis et al. [ 14] in Greece that showed 134 of 290 residents (51%) experienced a high level of burnout in at least one aspect of PA, DP, or EE, 48 residents (18.3%) experienced it in a combination of two aspects, and 13 residents (4.9%) had it in all three domains. The current study also showed the QoL of residents. The participants’ average QoL scores of each domain (1–4) are 63.24, 65.85, 62.58, and 63.06, respectively. Age is found to be a significant influence on all QoL domains, whereas emergency cases and death significantly influence psychological and social relations domains. Lourenção et al. [ 9] found a high rate of health problems impairing residents’ QoL and consequently, quality of care provided to patients. A study by Macedo et al. [ 15] discovered the residents’ QoL in terms of vitality, social life, emotional life, and mental health was comparable to patients with chronic conditions. However, Whang et al. [ 16] discovered that most residents experienced improved QoL while adhering to the working hour limits. The study findings also revealed the correlation between EE and physical health in which burnout and QoL (physical domain) are inversely correlated. Another study has also shown that first year residents underwent changes in their QoL due to burnout. The burnout relates to the responsibilities and workload as residents. Thus, residents require psychological support and stresscoping to cope with burnout and improve the QoL during residency [ 17]. Dyrbye and Shanafelt [ 18] also reported similar results on general practitioners. Meanwhile, Naz et al. [ 19] stated that poor QoL is strongly associated with burnout, reduced work performance and early retirement. Burnout and QoL are likely to be influenced by numerous factors [ 19]. The current study has identified both intrinsic and extrinsic factors which either can cause or protect residents from burnout. The intrinsic causative factors include physical exhaustion, personality, motivational and time management. Previous studies stated that individuals experiencing physical exhaustion also report sleep disturbances. This shows that sleep disturbance may be more associated with an exhaustion component of burnout [ 14]. Good state of physical health may be difficult to be achieved by residents who work more than 80 hours per week since residency program is associated with chronic lack of sleep [ 20]. The residency program needs to be of the residents’ own choice and in line with the field of interest, because otherwise, the individual experiences a sense of compulsion to undergo all activies, resulting in burnout and decreased QoL. This is consistent with the findings of Malik et al. [ 21], stating the incidence of burnout is closely correlated with unhappiness with one’s profession, as well as a desire for a profession change. In terms of time management, residents experiencing burnout tend to complete tasks under suboptimal conditions and in a hasty manner. This is also reinforced by the findings from other studies showing that handover of assignments between residents is often carried out in less-than-optimal conditions, including within public places, often being interrupted, and without giving the recipients an opportunity to ask questions [ 17]. Intrinsically, protective factors include personality, coping stress, adequate rest, and spirituality. This is in accordance with the report from Dimitriu et al. [ 22] showing that optimism, high motivation, and extrovert personality are able to reduce personal anxiety and consequently prevent burnout. Spirituality is also identified as one of the inhibiting factors for burnout. Wachholtz and Rogoff [ 23] discovered that individuals with higher spirituality scores were less likely to experience severe burnout or depression. Individuals with high spirituality tend to describe a feeling of satisfaction with life in general [ 23]. A study by Estupiñan and Kibble [ 24] showed a significant inverse correlation between spirituality level and burnout incidence as well as between spirituality and cynicism. Thus, spirituality is a possible means of functional coping, through the search for meaning, purpose and hope in life, and able to replace cynicism as a coping mechanism, during burnout. However, no studies were found regarding the relationship between spirituality and burnout in the context of medical residents [ 24]. Nevertheless, institutions should consider providing spiritual support for residents or facilitating opportunities for residents to involve in spiritual activities, as one way to prevent burnout. Extrinsic factors are also divided into two, causative and protective factors. Causative factors include workload, working system, hierarchical working relationship, limited number of residents, and inadequate supporting facilities/equipment. Similar findings were obtained by Dyrbye and Shanafelt [ 18] which showed that burnout continued during transition from medical school to residency, especially in stage 1 (50%), and this was due to the heavier physical workload, compared to other stages, along with the adaptation process. A report by Fainberg and Lee [ 25] stated that 44% residents experienced burnout due to working over 80 hours per week, a significantly higher rate, compared to peers working less than 80 hours (24%). Furthermore, Gopal et al. [ 26] imposed an 80-hour work for a week and observed a decrease in all burnout subscales, especially EE. Limiting working hours is likely to be a measure to reduce burnout and thus, increase QoL of residents. The current study has identified that malfunctioning or unavailability of working facilities or equipment which interferes with work is likely to cause burnout. Ghavidel et al. [ 27] observed similar situation in the nursing profession. Inadequate equipment such as broken beds and supporting examination tools is one of the most significant recurring obstacles in the care environment resulting in distraction, neglected care, delays in providing care, EE, and absence from work [ 27]. To the best of the authors’ knowledge, no other studies are found in the residency context. However, this should not deter the institution from ensuring adequate facilities or equipment to minimize burnout. Several factors, namely institutional support system, peer support, and family support, are identified as extrinsic protective factor. According to Rogers et al. [ 28], in the workplace, medical colleagues are a potential source of support, in addition to family and friends. The study identified co-workers as a significant form of support for relieving work-related stress and burnout [ 28]. Participants also stated the importance of counseling facilities for preventing burnout. This is in line with the study of Fainberg and Lee [ 25] which showed that institutional factors, for example, access to psychological health services and formal counseling, are correlated with lower burnout rates. Putri et al. [ 29] provided suggestions for the institution to ensure residents have regular and reliable access to family doctors, psychologists, as well as psychiatrists. The current study has examined the relationships between burnout and QoL of residents. This implies that to obtain a high QoL, burnout needs to be minimized. Moreover, this study has identified the negative impact of burnout, which are underperformance and physical and psychological disorders. Therefore, it is essential for the institution to support residents through screening for burnout from the early stage, even at the admission, provision of support system and adequate infrastructure, regulation of working hours, and supportive supervision. A study in the Netherlands by Prins et al. [ 30] showed residents having a mutually supportive and beneficial relationship with supervisors have lower EE and DP scores, compared to residents feeling less valued by supervisors. Since there are both intrinsic and extrinsic factors which can either protect from or cause burnout, then it is important for residents to identify those factors. Personality type, motivation level, and the ability to balance time between work and personal life are some of the factors that need to be attended by the residents. The effort to minimize burnout and improve QoL goes both ways from the institution and the residents themselves. If spirituality was identified as one of the protective factors, thus residents need to enhance their spirituality to cope with the demands and burden of residency programs, but the institution needs to ensure that residents have the opportunity and time to do spiritual-related activities. This study is not without limitations, as the study was only conducted in one institution with six residency programs only. The study was also conducted during the coronavirus disease 2019 pandemic period and this possibly affected the participants’ condition when completing the questionnaire. However, the current study has shed light on the importance of reducing burnout to improve QoL and in the end, increase the quality of healthcare service. Further study exploring in even more depth the cultural factors related to residents’ burnout and QoL may be worthwhile.
In conclusion, one-third of residents in the current study experienced severe burnout. Several variables such as surgical program, difficult/rare cases, and working hours significantly correlate with certain domains of burnout. Residents’ QoL is proven to correlate with burnout domains. Each unit increase in burnout level decreases the residents’ QoL. Therefore, both residents and the institution need to work on reducing burnout and improving QoL. Residents can nurture good spirituality, strengthen the motivation, and involve in coping with stressful activities. While at the same time, institutions need to provide screening for burnout, regular psychological support, leisure activities, regulation of working hours, and supportive environment and working relationships. A reciprocal relationship between residents and the institution is required to minimize burnout and improve QoL.
Acknowledgments
The authors would like to thank all participants involved in this study.
Fig. 1.
Relationships between Themes and Subthemes
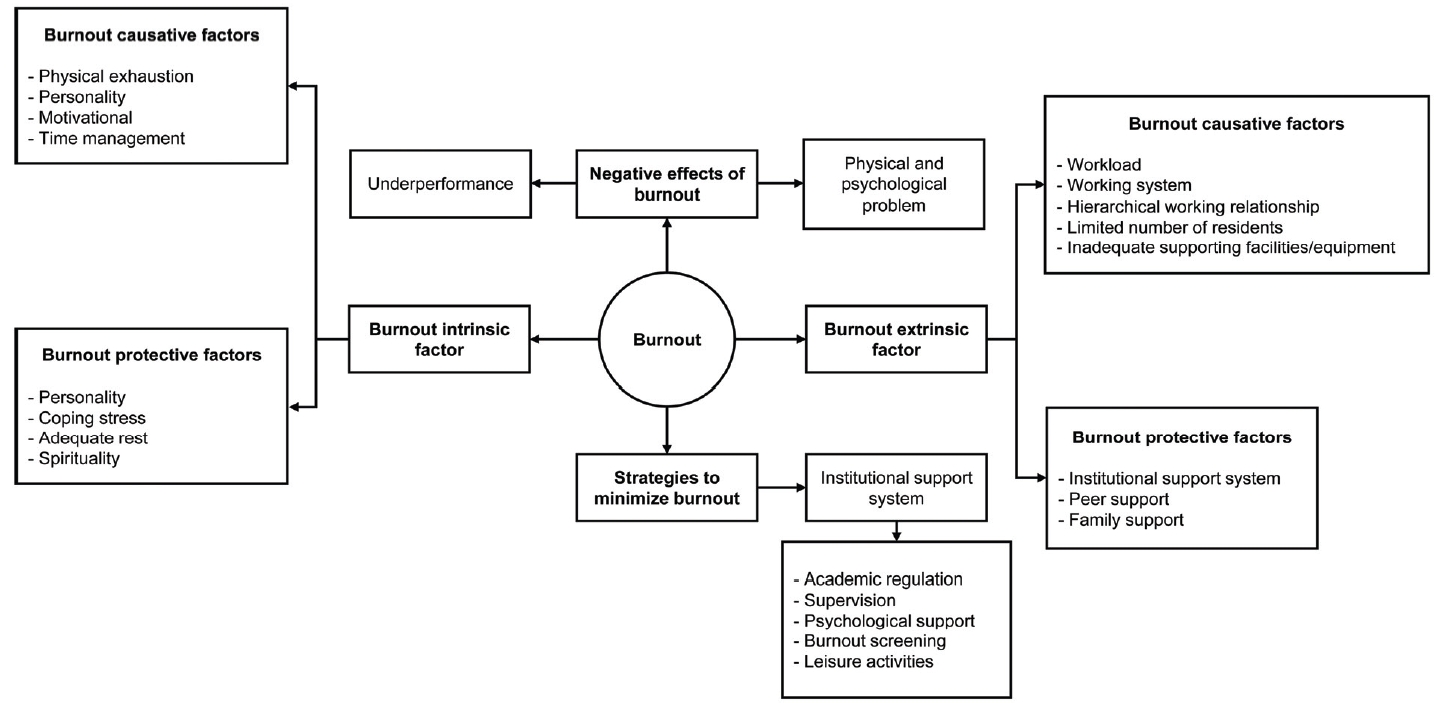
Fig. 2.
The Relationship between Variables Qualitatively and Quantitatively
EE: Emotional exhaustion, DP: Depersonalization, PA: Personal accomplishment.
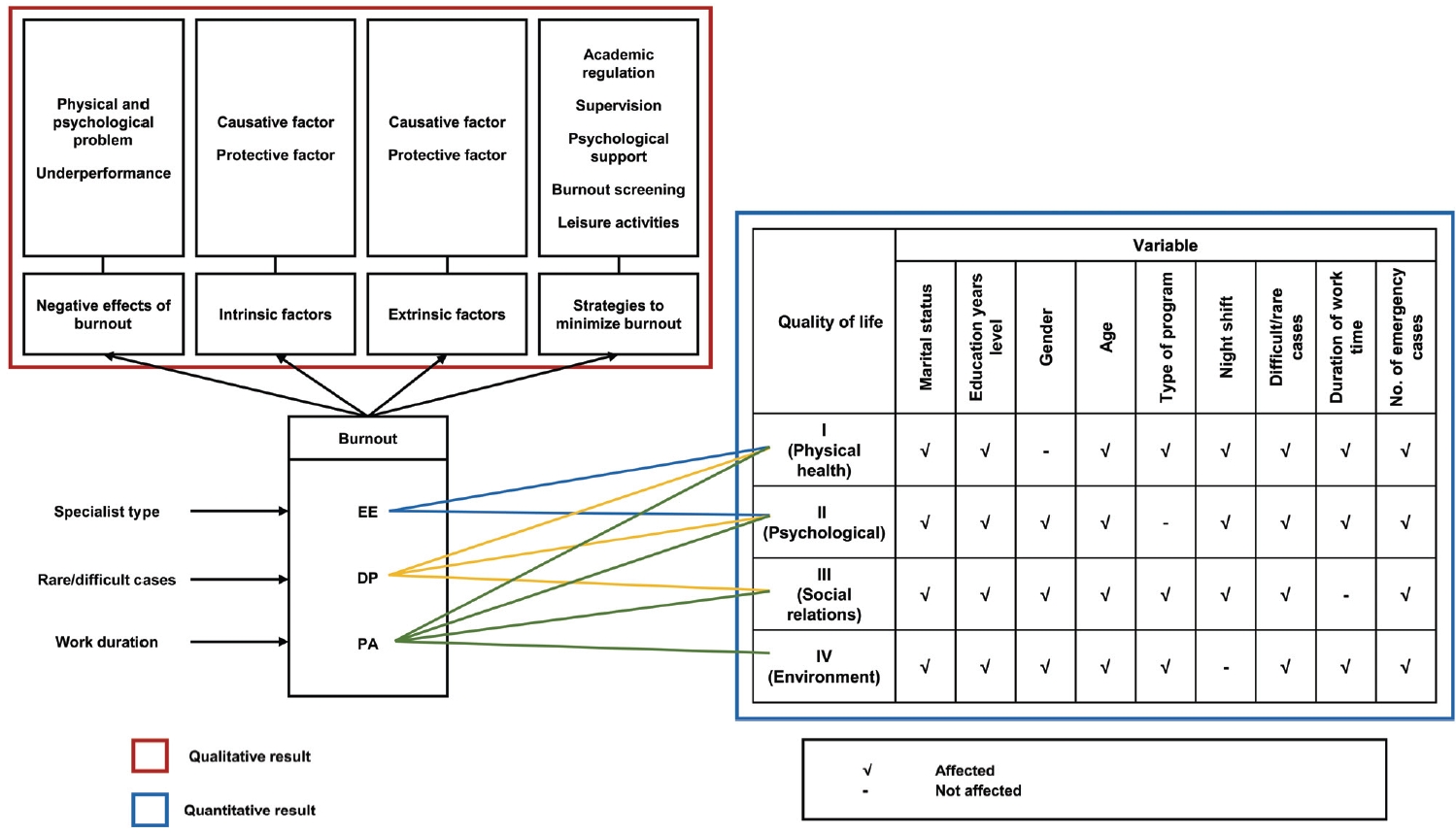
Table 1.
Characteristics of Study Participants, Distribution of Maslach Burnout Inventory Human Service Survey, and World Health Organization Quality of Life-BREF Scores (n=86)
|
Characteristic |
Value |
|
Gender |
|
|
Male |
48 (55.8) |
|
Female |
38 (44.2) |
|
Marital status |
|
|
Single |
28 (32.6) |
|
Married |
58 (67.4) |
|
Residency program |
|
|
Non-surgery |
40 (46.5) |
|
Surgery |
46 (53.5) |
|
Study phase |
|
|
First year |
35 (40.7) |
|
Second year/more |
51 (59.3) |
|
Age (yr) |
31±2.8a)
|
|
No. of night shifts per week (hr) |
48 (24–108) |
|
No. of difficult/rare cases per week (cases) |
2 (0–10) |
|
No. of working hours per week (hr) |
96 (68–216) |
|
No. of emergency cases and deaths per week (cases) |
6 (0–50) |
|
Emotional exhaustion domain |
|
|
Low |
34 (39.5) |
|
Moderate |
25 (29.1) |
|
Severe |
27 (31.4) |
|
Depersonalization domain |
|
|
Low |
43 (50.0) |
|
Moderate |
21 (24.4) |
|
Severe |
22 (25.6) |
|
Personal accomplishment domain |
|
|
Low |
40 (46.5) |
|
Moderate |
18 (20.9) |
|
High |
28 (32.6) |
|
Quality of life domain 1 (physical health) |
63.24±13.8a)
|
|
Quality of life domain 2 (psychological) |
65.85±13.8a)
|
|
Quality of life domain 3 (social) |
62.58±15.7a)
|
|
Quality of life domain 4 (environment) |
63.06±12.1a)
|
Table 2.
Factors Related to Burnout and QoL
|
Variable |
Burnout domain (logistic regression)
|
Beta coefficient on QoL domain (linear regression)
|
|
EE |
DP |
PA |
Physical (domain 1) |
Psychological (domain 2) |
Social (domain 3) |
Environment (domain 4) |
|
Related factors |
|
|
|
|
|
|
|
|
|
Age |
NS |
NS |
NS |
0.813 |
-0.29 |
0.30 |
0.10 |
|
No. of working hours per week |
NS |
NS |
1.03 |
-0.07 |
-0.06 |
NS |
0.01 |
|
No. of night shifts per week (hr) |
NS |
NS |
NS |
0.23 |
0.28 |
0.16 |
NS |
|
No.of emergency and deaths per week (cases) |
NS |
NS |
NS |
-0.21 |
0.15 |
0.07 |
0.39 |
|
No. of rare/difficult cases |
NS |
1.14 |
NS |
1.280 |
0.32 |
0.61 |
-0.63 |
|
QoL |
|
|
|
|
|
|
|
|
|
Physical |
NS |
NS |
NS |
- |
-a)
|
- |
- |
|
|
Psychological |
0.91 |
NS |
NS |
- |
- |
- |
- |
|
|
Social |
NS |
NS |
NS |
- |
- |
- |
- |
|
|
Environment |
NS |
NS |
NS |
- |
- |
- |
- |
|
Constant |
|
|
|
33.38 |
65.58 |
33.88 |
49.31 |
|
Categorical data |
|
|
|
|
|
|
|
|
Gender |
|
|
|
|
|
|
|
|
|
Male |
NS |
NS |
NS |
NS |
Refb)
|
Ref |
Ref |
|
|
Female |
NS |
NS |
NS |
NS |
-2.89 |
3.2 |
2.52 |
|
Type of residency program |
|
|
|
|
|
|
|
|
|
Non-surgery |
Ref |
NS |
NS |
Ref |
Ref |
Ref |
Ref |
|
|
Surgery |
2.65 |
NS |
NS |
2.98 |
NS |
5.98 |
6.01 |
|
Marital status |
|
|
|
|
|
|
|
|
|
Single |
NS |
NS |
NS |
Ref |
Ref |
Ref |
Ref |
|
|
Married |
NS |
NS |
NS |
-5.046 |
-3.145 |
3.69 |
-2.30 |
|
Phase of study |
|
|
|
|
|
|
|
|
|
First year |
NS |
NS |
NS |
Ref |
Ref |
Ref |
Ref |
|
|
Second year/more |
NS |
NS |
NS |
4.233 |
7.57 |
4.92 |
5.84 |
|
EE |
|
|
|
|
|
|
|
|
|
Low |
- |
- |
- |
Ref |
Ref |
Ref |
Ref |
|
|
Moderate+severec)
|
- |
- |
- |
-3.5 |
-8.1 |
NS |
NS |
|
DP |
|
|
|
|
|
|
|
|
|
Low |
- |
- |
- |
Ref |
Ref |
Ref |
Ref |
|
|
Moderate+severe |
- |
- |
- |
-1.8 |
-1.9 |
-4.3 |
NS |
|
PA |
|
|
|
|
|
|
|
|
|
Low+moderate |
- |
- |
- |
Ref |
Ref |
Ref |
Ref |
|
|
High |
- |
- |
- |
4.3 |
5.6 |
3.7 |
2.5 |
Table 3.
|
Participant |
Gender |
Age (yr) |
Marital status |
Residency program |
Semester |
Burnout level
|
|
EE |
DP |
PA |
|
RESP-1 |
M |
35 |
Married |
Pulmonology |
1 |
Low |
Moderate |
Low |
|
RESP-2 |
F |
28 |
Single |
Internal Medicine |
3 |
Severe |
Moderate |
Moderate |
|
RESP-3 |
M |
29 |
Single |
Internal Medicine |
4 |
Severe |
Low |
Low |
|
RESP-4 |
M |
31 |
Married |
Anesthesiology |
2 |
Severe |
Severe |
High |
|
RESP-5 |
F |
31 |
Married |
Anesthesiology |
1 |
Moderate |
Severe |
Low |
|
RESP-6 |
F |
36 |
Married |
Pediatric |
5 |
Low |
Low |
High |
|
RESP-7 |
M |
31 |
Married |
Surgery |
2 |
Moderate |
Severe |
High |
|
RESP-8 |
F |
27 |
Married |
Obstetrics & gynecology |
3 |
Moderate |
Moderate |
Low |
|
RESP-9 |
M |
30 |
Married |
Surgery |
3 |
Moderate |
Severe |
Low |
|
RESP-10 |
F |
28 |
Single |
Obstetrics & gynecology |
1 |
Severe |
Low |
Moderate |
References
1. Ishak WW, Lederer S, Mandili C, et al. Burnout during residency training: a literature review. J Grad Med Educ 2009;1(2):236-242.   2. Ebrahimi S, Kargar Z. Occupational stress among medical residents in educational hospitals. Ann Occup Environ Med 2018;30:51. 3. Faivre G, Marillier G, Nallet J, Nezelof S, Clment I, Obert L. Are French orthopedic and trauma surgeons affected by burnout?: results of a nationwide survey. Orthop Traumatol Surg Res 2019;105(2):395-399. 4. Zheng H, Shao H, Zhou Y. Burnout among Chinese adult reconstructive surgeons: incidence, risk factors, and relationship with intraoperative irritability. J Arthroplasty 2018;33(4):1253-1257. 6. Theofilou P. Quality of life: definition and measurement. Eur J Psychol 2013;9(1):150-162. 7. Maslach C, Jackson S, Letter M. Maslach Burnout Inventory Manual. 3rd ed. Palo Alto, USA: Consulting Psychologists Press; 1996.
9. Lourenção LG, Moscardini AC, Soler ZA. Health and quality of life of medical residents. Rev Assoc Med Bras (1992) 2010;56(1):81-91.  10. AbdAllah AM, El-Hawy LL. Burnout and health related quality of life among resident physicians in Zagazig University Hospitals. Egypt J Occup Med 2019;43(2):189-204. 11. West CP, Shanafelt TD, Kolars JC. Quality of life, burnout, educational debt, and medical knowledge among internal medicine residents. JAMA 2011;306(9):952-960. 12. Dahlan MS. Besar sampel dan cara pengambilan sampel dalam penelitian kedokteran dan kesehatan [Sample size and methods in medical and health research]. 3rd ed. Jakarta, Indonesia: Salemba Medika; 2012.
15. Macedo PC, Cítero Vde A, Schenkman S, NogueiraMartins MC, Morais MB, Nogueira-Martins LA. Health-related quality of life predictors during medical residency in a random, stratified sample of residents. Braz J Psychiatry 2009;31(2):119-124. 17. Block L, Wu AW, Feldman L, Yeh HC, Desai SV. Residency schedule, burnout and patient care among first-year residents. Postgrad Med J 2013;89(1055):495-500. 18. Dyrbye L, Shanafelt T. A narrative review on burnout experienced by medical students and residents. Med Educ 2016;50(1):132-149. 19. Naz S, Hashmi AM, Asif A. Burnout and quality of life in nurses of a tertiary care hospital in Pakistan. J Pak Med Assoc 2016;66(5):532-536. 20. Prins JT, Gazendam-Donofrio SM, Tubben BJ, van der Heijden FM, van de Wiel HB, Hoekstra-Weebers JE. Burnout in medical residents: a review. Med Educ 2007;41(8):788-800. 24. Estupiñan B, Kibble J. The relationship between spirituality and burnout in the lives of medical students. Med Sci Educ 2018;28(1):37-44. 26. Gopal R, Glasheen JJ, Miyoshi TJ, Prochazka AV. Burnout and internal medicine resident work-hour restrictions. Arch Intern Med 2005;165(22):2595-2600. 28. Rogers E, Polonijo AN, Carpiano RM. Getting by with a little help from friends and colleagues: testing how residents’ social support networks affect loneliness and burnout. Can Fam Physician 2016;62(11):e677-e683. 29. Putri IA, Soedibyo S. Tingkat Depresi Peserta Program Pendidikan Dokter Spesialis Ilmu Kesehatan Anak FKUI-RSCM dan Faktor-Faktor Terkait [The level of depression of pediatric residents in FKUI-RSCM and its associated factors]. Sari Pediatr 2016;13(1):70.
30. Prins JT, Gazendam-Donofrio SM, Dillingh GS, van de Wiel HB, van der Heijden FM, Hoekstra-Weebers JE. The relationship between reciprocity and burnout in Dutch medical residents. Med Educ 2008;42(7):721-728.
|
|











