Cardiology residents’ attitudes towards clinical supervision: a multi-centered study
Article information

Abstract
Purpose
Residents’ gender, residency level, and hospital types might influence their attitudes towards clinical supervision (CS); however, reports of its impact on cardiology residency are nonexistent. We explore the effect of gender, residency level, and hospital location’s effect on Indonesian cardiology trainees’ attitudes towards CS.
Methods
A multi-centered, cross-sectional study was conducted. We invited 490 Indonesian cardiology residents in September– October 2019 to complete the Cardiology CS Scale. Residents’ attitudes, gender, university, and residency year were expressed using descriptive statistics. A Mann-Whitney test analyzed the gender and university location effect on residents’ attitudes. Training year and university’s impact were subjected to the Kruskal-Wallis test; a p-value of <0.05 reflected a significant result.
Results
A total of 388 residents agreed to participate (response rate=79.18%). Most of them were male (n=229 [59,02%]), attended universities in Java Island (n=262 [67,52%]), and were in their 2nd–3rd year of training (n=95 [24.48%], each). There were no significant differences in residents’ attitudes between genders (U [Nmale=229, Nfemale=159]=17,908.50, z=-0.27, p=0.78). Generally, their attitudes were significantly affected by the university (H(7)=47.38, p<0.01). However, the university location (located in Java Island or outside Java Island) does not affect residents’ attitude towards CS (U [NJava=262, Nnon-Java=126]=15,237.00, z=-1.23, p=0.22). In addition, the residents’ training year also affected the residents’ response (H(2)=14.278, p<0.01).
Conclusion
Cardiology residents’ attitudes towards CS are significantly influenced by training year and university but not gender or university location. The results might provide insightful information for further improvement of CS in cardiology training and guide further evaluation.
Introduction
Evaluating clinical supervision (CS) is crucial as it promotes residents’ independence, ensures patients’ safety, and prepares the residents to be future supervisors [1-4].
However, to our knowledge, no study has been conducted to evaluate CS conducted specifically in cardiology residency, which, to some extent, is unique compared to those in the medical cluster residency. Unlike internal medicine, cardiology has a narrow yet comprehensive and deep focus [5,6]. Besides, although this residency is procedural-heavy, the residents are deemed competent in medical practice and non-invasive imaging [7]. This fact might affect the CS given in cardiology residency and the perceived quality of CS from the residents’ point of view [6].
Resident-filled questionnaires are often used to measure the quality of CS from the residents’ view. The Cardiology Clinical Supervision Scale (CCSS) has been developed in cardiology residency to evaluate CS from cardiology residents’ view. It has been validated and provided sufficient evidence of validity and reliability (e.g., content validity, structural validity, and internal consistency) [8]. Using different scales and residency populations, studies have investigated variables affecting residents’ attitudes towards CS, including gender, residency year, and hospital types. Studies revealed no significant correlation between gender and residents’ attitudes toward CS [9,10]. Residents’ level affects their attitudes in several studies, in which more positive attitude was recorded from junior residents compared to the ‘senior’ colleagues [11,12]. As for the hospital type, studies found a more positive attitude from those trained in a district hospital [13,14]. However, mixed results regarding the correlation of such variables with the responses toward CS are also reported [15,16]. The information obtained can be used as an analysis to shape the residency program and develop better residency and CS for the cardiology residency.
This study aims to investigate cardiology residents’ attitudes toward CS and explore the effect of their gender, clinical year, and university on their attitudes toward CS.
Methods
1. Study settings
Indonesia has 13 state-owned universities conducting cardiology residency programs in their affiliated state-owned hospital (national and provincial hospitals). Seven universities are located on Java Island, the archipelago’s most populated [17]. Other six universities are spread among the other islands: Sumatra Island (three universities), Bali Island (one university), and Sulawesi Island (two universities). The postgraduate cardiology training in Indonesia is structured as a 4-year program where the residents rotate to sub-divisions in the cardiology department, internal medicine, thoracic, cardiac, and vascular surgery department/division, radiology and nuclear medicine department, and pediatric department [5]. In each rotation, the residents (or group of residents) will be assigned a supervisor (with a ratio of 1:5 or one supervisor to five residents or less). Yet, they are encouraged to follow other consultants during their rotation to gain more knowledge and experience.
2. Study design and participants
A multi-centered, cross-sectional study was conducted. A total of 490 Indonesian cardiology residents from eight universities (five on Java Island and one from Sumatra, Bali, and Sulawesi Island each) were invited to participate between September and October 2019. For confidentiality, the universities were coded as universities A to H. Ethical approvals were obtained from the Research Ethics Committee of the University of Nottingham, the United Kingdom (ethics reference no., 234-1902) and Universitas Padjadjaran, Indonesia (ethics reference no., 610/UN6. KEP/EC/2019). To invite the resident to participate in this study, an invitation email with a unique JISC Online Survey link (JISC, Bristol, UK) was sent to each resident’s email, followed by four reminders. Besides, all contact persons whom each center appointed encouraged the residents to participate. Finally, all residents’ identification was deleted after data collection. Written informed consent was collected before the study, and participants knew their rights to withdraw at any study step.
3. Cardiology Clinical Supervision Scale
The CCSS was developed and validated to assess cardiology residents’ attitudes toward CS. The item of CCSS was developed from an extensive literature examination and conceptual framework of CS and was to be measured using a 5-level Likert Scale (i.e., 1=strongly disagree; 2=disagree; 3=neutral; 4=agree; 5=strongly agree). The content validity of CCSS has been evaluated by 10 experts qualitatively by providing their input, which helped us to improve the items, and quantitatively using the content validity index (G-coefficient=0.71) indicating their agreement upon the items’ validity. An exploratory factor analysis reduced the item to 19 variables, divided into two subscales: supervisory interaction and facilitation (SIF) (n=10 items) and role modeling (RM) (n=9 items). with an excellent Cronbach’s α reliability score (0.93 for SIF and 0.90 for RM) [8].
4. Data analysis
Descriptive and inferential statistics were run to understand cardiology residents’ attitudes toward CS and how gender, year of residency, and university affect their attitudes. Descriptive statistics were used to understand the residents’ attitudes towards CS, data distribution, and demographic information based on their gender, university, and residency year. Normally distributed data will be reported as mean±standard deviation, whereas those non-normally distributed data will be presented as median (interquartile range). The inferential statistics were used to investigate the association between the residents’ gender, university, residency year and their attitudes toward CS. Residency year was classified into three groups (i.e., early residency year [1st and 2nd year], final residency year [3rd and 4th year], and post-final year [5th and >5th year]). Besides the original classification, the universities were divided into those inside Java Island (n=5 universities) and other islands (n=3 universities).
Gender association with residents’ attitudes towards CS was subjected to Welch’s t-test or Mann-Whitney test. Residency year and university differences in residents’ attitudes were subjected to one-way analysis of variance or the Kruskal-Wallis test. Should we find a significant difference, a post hoc test will be conducted using the Bonferroni test to understand the interaction causing the significant differences. Finally, we analyzed the differences between universities in Java and outside Java using Welch’s t-test or Mann-Whitney test. All statistical analysis was conducted using IBM SPSS Statistics ver. 26.0 (IBM Corp., Armonk, USA).
Results
A total of 388 responses were collected (response rate=79.18%), in which most study participants were male (n=229 [59.02%]), with University F providing the highest response rate (90.79%; n=69 responses out of 76 residents). Most participants were from universities in Java (n=262 [67.52%]). Second- and third-year residents covered almost half of the participants in this study (n=95 [24.48%], each). When reallocated into three groups, those in the final year group (3rd–4th year) covered 43.04% (n=167) of the participants. Table 1 summarizes the demographic data of the study participants. A Kolmogorov-Smirnov test indicated that the overall residents’ attitudes towards CS do not follow a normal distribution (D(388)=0.13, p<0.01). Similar results were found for the data in SIF (D(388)=0.15, p<0.01) and RM (D(388)=0.17, p<0.01) subscales. The median score for the overall scale, SIF, and RM subscales were 3.95 (0), 3.80 (1), and 4.00 (0), respectively (Table 2).
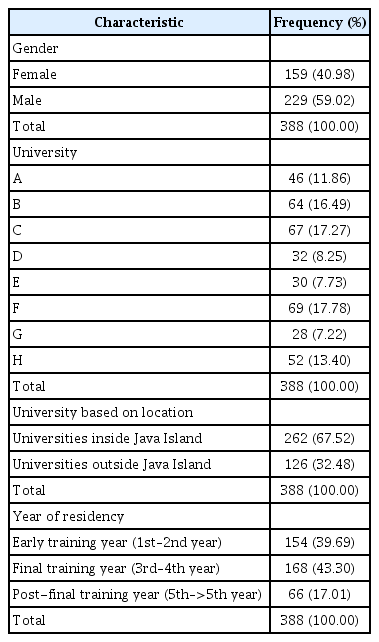
Demographic Profile of the Study Participants (n=388)

Descriptive Statistics of the Residents’ Attitudes towards Clinical Supervision (n=388)
1. Gender differences in CS
There was no statistically significant difference between male (median, 3.95; IQR, 0) and female (median, 3.95; IQR, 0) residents’ attitudes towards CS (U [Nmale=229, Nfemale=159]=17,908.50, z=-0.27, p=0.78). A similar result was yielded for each subscale: SIF (male: median, 3.80; IQR, 0; female: median, 3.80; IQR, 0; U [Nmale=229, Nfemale=159]=17,856.00, z=-0.32, p=0.75) and RM (male: median, 4.00; IQR, 0; female: median, 4.11; IQR, 0; U [Nmale=229, Nfemale=159]=18,032.00, z=-0.16, p=0.87) subscales.
2. Indonesian cardiology residents’ attitudes toward CS based on the university
Table 3 summarizes the descriptive analysis of the data based on the university. A Kruskal-Wallis test showed that university affected residents’ attitudes towards CS (H(7)=47.38, p<0.01). A post-hoc analysis using the Bonferroni study showed that the differences were caused by the interaction between universities F and B, F and C, F and E, A and C, and A and E (p<0.05), and the effect size test shows that the magnitude of the difference was medium (Epsilon-square=0.122). A further study based on each subscale also indicated a significant difference in SIF score (H(7)=37.87, p<0.01) and RM score (H(7)=43.98, p<0.01) between universities.

Descriptive Statistics of the Residents’ Attitudes towards Clinical Supervision by the University (n=388)
The universities were divided into those in Java Island (Universities B, C, D, E, and F) and other islands (University A, G, and H). A Mann-Whitney U test showed no statistically significant difference in residents’ attitudes between those trained in Java or outside Java (U [NJava=262, Nnon-Java=126]=15,237.00, z=-1.23, p=0.22). A similar result was found in SIF (U [NJava=262, Nnon-Java=126]=16,267.00, z=-0.23, p=0.82) subscale. However, there was a significant difference in the RM subscales score between the two groups (U [NJava=262, Nnon-Java=126]=13,571.50, z=-2.86, p<0.01).
3. Indonesian cardiology residents’ attitudes toward CS based on the residency year
Table 4 summarizes the descriptive statistics of the study participants based on their residency year. A Kruskal-Wallis test indicated that residency year influenced residents’ attitudes towards CS (H(2)=14.278, p<0.01). A post hoc analysis using Bonferroni analysis suggested that the interaction causing the differences was between the final and post-final year groups and between the early and post-final year groups (p<0.05). In contrast, the differences between the early-year and final-year groups were not statistically significant (p=0.21). Furthermore, the effect size test showed that the magnitude of the difference was small (Epsilon-square=0.04). A further study based on each subscale indicated that both SIF factor and RM factor are significantly different between the residency years (H(2)=17.07, p<0.01) for SIF and (H(2)=6.02, p<0.05) for RM factors.
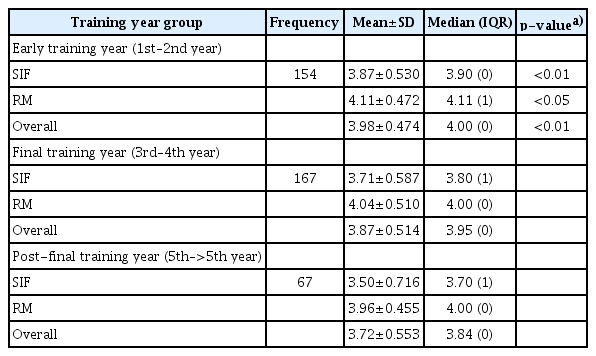
Descriptive Statistics of the Residents’ Attitudes towards Clinical Supervision by Training Year (n=388)
Discussion
This study was the first to utilize the newly developed CCSS scale. Therefore, a discussion should be created cautiously, as other studies used different instruments. The median score for Indonesian cardiology residents’ attitudes towards CS indicated that most of the residents had a positive attitude towards CS and similar results were found in both subscales (SIF: median, 3.80; IQR, 1; RM: median, 4.00; IQR, 0). These results may indicate that CS conducted in cardiology residency in Indonesia has been well structured and delivered, which should be maintained, improved, and evaluated regularly.
This study was the first to use CCSS to measure cardiology trainees’ attitudes towards CS. To our knowledge, this is the first study specifically reporting this topic in such a population. Beckman et al. [6] in 2006 have reported the uniqueness of CS in cardiology training as they found that cardiology trainees cannot differentiate between the supervisors’ interpersonal and clinical teaching abilities in the CS process. This was assessed mainly due to typical patients encountered by a cardiologist and their learning environment. However, they did not report their attitudes towards CS [6], as reported in our study. Besides, we have not found any study measuring CS evaluation in any residency program in Indonesia; thus, this study is also the first to study this topic in Indonesia.
1. How residents’ gender affects their attitudes towards CS
Gender does not affect cardiology residents’ attitudes toward CS in this study. Although no studies have been conducted in such populations (cardiology residents and Indonesians), earlier studies on this matter have been controversial. For example, Jochemsen-van der Leeuw et al. [18] reported that general practice residents’ gender did not affect how they rated their clinical trainer as a role model in the CS process. Similarly, Fluit et al. [13] conducted a study on residents in 15 disciplines and found insignificant differences in residents’ evaluation of clinical teaching between genders. However, they reported that residents’ gender influences their attitudes towards their supervisor as a role model [13]. In this study, however, no difference was found in the RM subscale.
In contrast to the reports above, a study indicated that student-preceptor gender interaction might affect medical students’ perception of their preceptors [19]. Although with a small, and negligible effect size, McOwen et al. [20] suggested that gender interaction might affect the evaluation of clinical teaching. Insignificant differences between genders in this study might indicate gender equality in the CS conducted in Indonesian cardiology residency.
2. Training years and its effect on residents’ attitudes towards CS
It might be usual to see residents’ attitudes towards CS differ between residency years. However, the declining score among advanced residents is worth noting. A statistically significant difference was found among the residency year groups, with those in more advanced residencies tend to give a lower score. To some extent, this result is per those reported by Fluit et al. [13], who conducted a study on residents from 15 different residency disciplines. No research, to the best of our knowledge, reported an opposing finding regarding this topic. Several explanations might be proposed. First, the supervision may use a fit-for-all approach, in which the supervisors deliver the supervision similarly for all residency levels. The importance of a tailored approach has been emphasized in the literature [11]. A fit-for-all approach might be unsuitable for each residency level’s current needs and ability. Literature has reported that early-year residents demand supervisor-directed learning, whereas seniors ask for more autonomy and resident-directed learning [11]. When unmet, residents might have less positive attitudes and provide a negative evaluation. Secondly, this phenomenon might be caused by the tendency of more senior residents to be more cautious and critical [13]; thus, a lower score can be obtained despite the maintained quality of the supervision.
3. University and its effect on residents’ attitudes towards CS
The median score of the residents’ attitudes was different across universities. The median score ranged between 3.79 (1) (University F) to 4.11 (0) (University C). A statistically significant difference was found between universities with a medium effect size. A similar result was also found in the analysis of both subscales. To our knowledge, there is no similar study in the literature. Two research compared CS conducted in university and district/affiliated hospitals as viewed by their residents [13,21]. Both studies agreed that residents’ attitudes were more positive for CS provided in the district hospitals than those in the university hospital. The possible explanation was that clinical teaching/supervision might receive a second priority in the academic hospital, lower than what is given to scientific research. No study reported a similar result as we compared similar types of hospitals (university hospitals) across the country. District hospitals are only regarded as satellite teaching hospitals and were not analyzed in this study. We compared universities located on Java Island and other islands. We found no significant difference between their overall attitudes towards CS and how they value the supervisory interaction and facilitation conducted. However, the difference was significant in the RM factor. Several items in the RM factors of the CCSS showed the supervisors’ role models as clinical supervisors, which might interchange with their ability to deliver supervision (SIF factor). It warrants further investigation whether this difference is related to the supervisors’ role modelling process as practicing doctors and to what extent it affects the residents’ attitudes.
4. Study limitation, implications, and further research
This study was the first to report Indonesian cardiology residents’ attitudes toward CS using a newly developed CCSS scale. However, despite its novelty, there are several limitations to reporting. First, as this study used a self-administered questionnaire, the possibility of social desirability bias was inevitable. The residents could be reluctant to provide a lower score for their CS despite the complete confidentiality provided. Additionally, Indonesian culture, which is presented as a country with high power distance and collectivistic value, might affect their assessment [22]. Secondly, this study was cross-sectional and thus might not show any causal relationship between the variables and cardiology residents’ attitudes towards CS. Further, this study cannot explain the differences among different demographic profiles. This study might provide information on which factor, within the CCSS’ factors, has a significantly different value between demographic profiles. However, it cannot explain the causes or which has more effect on the differences.
To the best of our knowledge, our study was the first to describe the factors affecting CS in cardiology residency and to use CCSS as a measurement tool. The information might provide insight to the faculty in their teaching and supervision and the education providers to improve their residency program. This study also opens the door for further studies regarding this topic. There are several recommendations for further studies ahead. First, there is a possibility for more demographic profiles to be studied regarding their effect on CS using CCSS. Secondly, conducting a longitudinal study to investigate the progress of the residents’ attitudes towards CS during the residency process is recommended. Further studies might use CCSS for the evaluation of any intervention on CS. Further studies using different methods to find a clear explanation for the differences in residents’ attitudes across residency years and universities are warranted. Lastly, CCSS might be adapted to allow its use in different specialties to provide information regarding this topic in other residency programs, specifically in Indonesia and other countries.
5. Conclusion
Indonesian cardiology residents have relatively positive attitudes towards their CS, which might imply an appropriate practice of CS. The fact that male and female residents score similarly provides insight into gender equality. However, a lower score given by senior residents was noteworthy. Concerns should be focused on whether the supervision is appropriate for the senior years. The differences between residents’ attitudes among universities might provide insight for national coordinators of cardiology training to standardize their training program. A more detailed standard on CS might be helpful, yet should not hinder the independence of each campus from providing supervision according to their needs and availability.
Acknowledgements
We thank the Collegium of Cardiology and Vascular Medicine Indonesia for their recommendation and support. Our highest appreciation to the Department of Cardiology and Vascular Medicine and the residents who participated in this study. We thank the government of Republic Indonesia for their support through the Indonesia Endowment Fund for Education (LPDP) as scholarship provider for IJTA. The abstract of this manuscript has been presented as a poster presentation at the 14th Jakarta Meeting on Medical Education (JAKMED) 2022.
Notes
Funding
The Government of Republic Indonesia supported this study through the Indonesia Endowment Fund for Education (LPDP) as scholarship provider for IJTA.
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Author contributions
Concepting or design of the work: IJTA, AF, AS, MI. Ethics acquisition: IJTA, MI. Data collection: IJTA, AS, MI. Data analysis: IJTA, AF, AS. Drafting the article: IJTA, AF. Critical revision and final approval: IJTA, AF, AS, MI.