The change of the COVID-19 pandemic on medical education in Korea: a national survey of medical schools
Article information

Abstract
Purpose
This study aims to investigate how medical schools in Korea managed their academic affairs and student support in response to the coronavirus disease 2019 (COVID-19) pandemic and their plans for the post-COVID-19 era.
Methods
An online survey was conducted, and a link to a questionnaire was distributed to all the administrators of the 40 medical schools in Korea. The final analysis data involved responses from 33 medical schools and 1,342 students. Frequency analysis, cross-tabulation analysis, Fisher’s exact test, and one-way analysis of variance were applied for statistical analysis.
Results
Regarding instruction methods, most medical schools in Korea transitioned from in-person learning to video-on-demand learning (51.5%) and real-time online learning (42.4%). Among the school leaders, 36.4% planned to continue offering online classes combined with in-person classes beyond the end of the pandemic. Among the students, the online class concentration and participation score was 3.0 points or lower, but the class understanding score was 3.6 points, above a moderate level.
Conclusion
Students cited the shorter times needed to attend school and being able to take classes repeatedly as advantages of online classes, and over one-third of medical schools intended to continue with a hybrid of in-person and online learning even after the COVID-19 pandemic restrictions end.
Introduction
In response to the rapid spread of coronavirus disease 2019 (COVID-19) across Korea from February 2020, the Ministry of Education recommended that medical schools discontinue all current course activities and postpone classes [1]. In response to this recommendation, medical schools that had already begun classes decided to discontinue or postpone lectures and clinical clerkships. However, the consensus was that classes could not be postponed further because it was necessary to follow the academic calendar and the schedule for the Korean Medical Licensing Examination; to accommodate the preexisting schedule, each medical school shifted from in-person to online classes and reduced opportunities for clinical clerkship or in-person clinical clerkship courses [2]. Online classes have been operated through video-on-demand (VOD) learning, real-time online learning, and online experiments and practice [3], and some clinical clerkship courses have been replaced with alternative activities [4-6]. In response to the prolonged COVID-19 infection conditions, the Korea Association of Medical Colleges (KAMC) distributed the “Guidance for medical students’ responses to COVID-19 in Korea” to Korea’s 40 medical schools in December 2020 to guide schools on continuing operations (lectures, assessments, administrative support, and so forth) during the pandemic conditions [7].
The COVID-19 pandemic and associated restrictions brought about the first implementation of online coursework in Korea’s medical schools. However, the issues brought about by this implementation were not unique to Korea; medical schools in every country reduced or suspended all in-person curriculum activities and switched to online coursework [3]. These conditions created ample opportunities for researchers to study the challenges, opportunities, and current conditions related to online classes in the COVID-19 environment at individual schools [8] and nationally [9].
In Korea as elsewhere, administrators at individual colleges assessed how best to maintain operations and meet students’ needs while adhering to COVID-19 pandemic restrictions on in-person academic activities. However, there has not to date been an examination of how medical schools nationwide responded to the pandemic restrictions. Against this backdrop, circumstances like the COVID-19 pandemic can lead to significant academic gaps for students. There is a need to understand how medical schools responded to the academic crisis and how well students adapted to emergency learning measures. Prolonged academic gaps can impact the annual supply of medical professionals and have macro-level implications for public health. Therefore, this study has two main objectives. Firstly, the study aims to investigate how schools first responded to the spread of infectious diseases like COVID-19, with the purpose of gathering foundational data for establishing future crisis response systems. Secondly, considering the uncertainty surrounding the possibility of resuming in-person classes for the semester after a delay of more than a month, the study aims to assess the success of the swift transition to emergency online learning. This transition was adopted as an alternative to in-person classes. The study also assesses whether the classes were effective, while also exploring the potential of online education post-COVID.
METHODS
To achieve this study’s aim, we administered a nationwide cross-sectional survey of students and administrators to all 40 medical schools in Korea. We administered the survey from April 26 to May 20, 2021, and received responses from a total of 33 medical school administrators and 1,344 premedical and medical students; from the latter, we excluded one student who did not give consent and one whose answers did not appear to be sincere. We used G*Power ver. 3.1.9.7 (Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany; http://www.gpower.hhu.de/) to calculate the minimum student sample size for analysis because it was difficult to practically identify the source population. The necessary sample size for students was 324 persons when recalculated with six-group one-way analysis of variance (ANOVA), 95% confidence level, 5% margin of error, and effect size 0.25 (medium). The number of student respondents exceeded the necessary sample size calculated.
We developed the questionnaires for school administrators (one designated from each school) with reference to previous studies on online class experiences during the COVID-19 pandemic [9] and based on interviews with two physicians. The school questionnaire had 38 questions, consisting of only nominal scales: seven questions related to COVID-19 experiences, nine regarding online classes and management of academic affairs, 12 on student guidance and support, seven on student assessment, and three on teaching development. A representative of each school was asked to answer this questionnaire. The student questionnaire consisted of 31 questions (25 items rated on a 5-point scale, Cronbach’s α=0.992); there were five questions on online class experiences, 24 on satisfaction with online lectures and practices, and two regarding opinions on the post-COVID-19 direction of medical education.
In developing the study questionnaire, seven experts conducted four rounds of assessments for content validity: three who specialized in education and one each from neuropsychiatry, internal medicine, pediatrics, and family medicine; all experts were working at medical schools at the time. The most common way to verify content validity is a panel of experts [10], and Lynn [11] recommends a panel of five to 10 experts; we selected seven as panel members. The panel members discussed and refined the questionnaire items until they reached consensus on for each item; the agreed-upon items showed calculated content validity indices of 0.78 or higher [12].
The surveys were administered via a Google Forms link (Google LLC, Mountain View, USA), and only respondents who gave online consent at the beginning of the survey could complete it. All respondents were asked to answer each question only once. To guarantee anonymity, we did not collect any identifying information, but participants were invited to provide their email addresses if they wished to receive a gift coupon in return for completing the survey. Following the surveys, we analyzed the responses from the medical school administrators and students using frequency analysis, cross-tabulation analysis, Fisher’s exact test, and one-way ANOVA to analyze the differences in students’ satisfaction with various instructional methods.
We performed all statistical analyses using IBM SPSS Statistics for Windows ver. 25.0 (IBM Corp., Armonk, USA). The present study protocol was reviewed and approved by the institutional review board of Kyungpook National University Hospital (approval no., KNU-2021-0053). Informed consent was submitted by all subjects when they enrolled.
RESULTS
1. General characteristics of the respondents
Table 1 gives the general characteristics of the 33 medical schools and 1,342 premedical and medical school students who answered the questionnaires.

General Characteristics of Survey Respondents
2. School responses to COVID-19 pandemic measures
Table 2 outlines how the medical school leaders in this study responded to and accommodated Korea’s nationwide COVID-19 infection control restrictions (e.g., managing academic affairs, staffing online classes, and securing partnerships with hospitals for clinical clerkships).
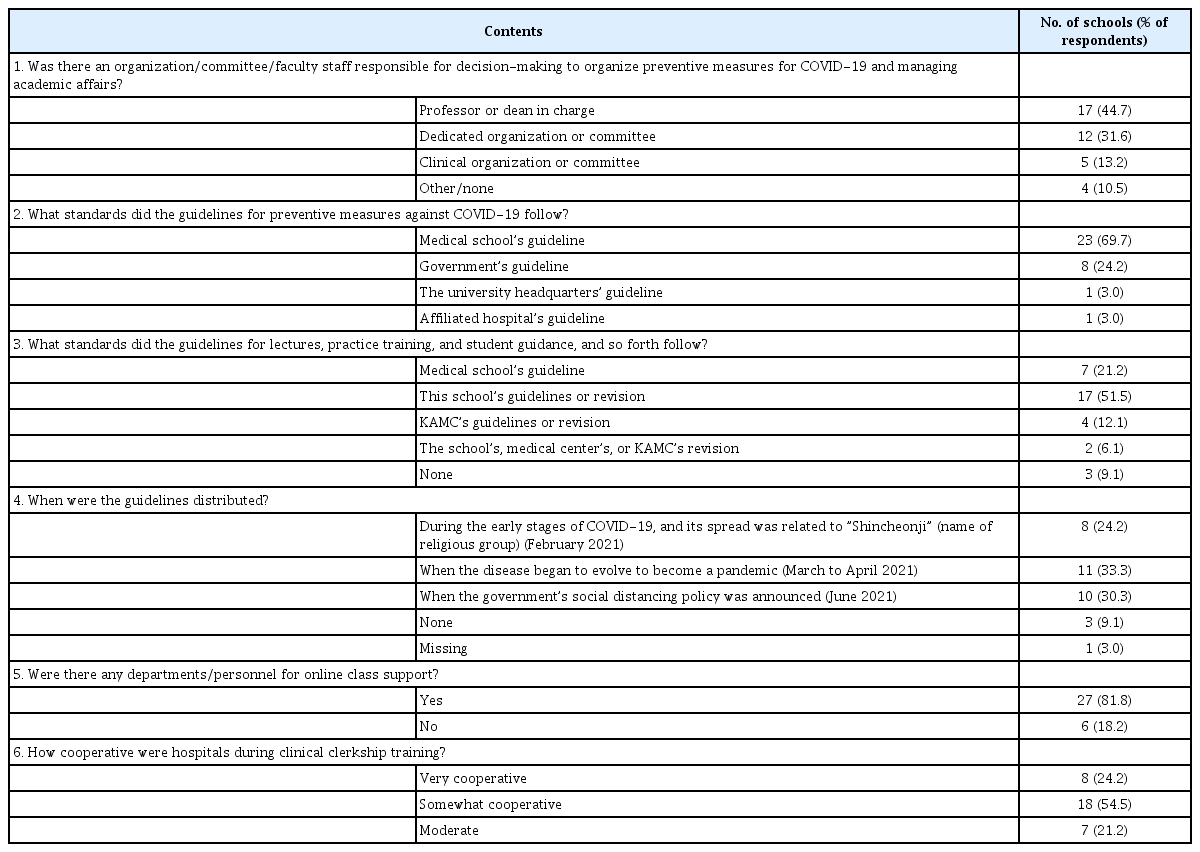
How Did School Leaders Operate under COVID-19 Restrictions?
Among the 33 medical schools, the responsibility of decision-making regarding COVID-19 prevention and academic operations was predominantly carried out by responsible professors or deans (44.7%). This was followed by dedicated teams or committees, which accounted for 31.6%. About 70% of the responding medical schools developed their own guidelines for COVID-19 prevention measures. However, for class and academic guidelines, the most common response (51.5%) indicated adherence to the university headquarters’ guidelines. The distribution of COVID-19 prevention guidelines primarily took place preemptively between February and April, before the government announced social distancing measures in June 2021. During this period, 19 medical schools (57%) distributed their self-developed guidelines. Regarding the transition to online classes, 27 medical schools (81.8%) allocated resources and personnel to support the transition, and 26 medical schools (79.7%) reported smooth cooperation with hospitals for clinical training during the COVID-19 pandemic.
The Fisher’s exact test results indicated no significant differences among schools in the number of students, the organization forms, the regional timing of developing and releasing guidance on preventive measures against COVID-19 and guidelines on managing academic affairs, the staffing of online classes, or the cooperation of hospitals for clinical clerkships.
3. Curriculum changes to accommodate COVID-19 pandemic restrictions
Regarding the medical schools’ online instruction methods, 52% of the responding administrators mainly provided video lectures, and 42% focused on real-time online classes (Table 3). The platform most commonly used in real-time classes was Zoom (Zoom Video Communications Inc., San Jose, USA) (68%). Medical schools decided (36%) or considered deciding (61%) to simultaneously operate in-person and online classes even after the end of the COVID-19 pandemic.

Online Classes and Management of Academic Affairs
For the basic medical science practice, online and in-person classes were combined (73%), and 25% of the administrators reported that the clinical training curriculum had been the most difficult to operate; most of the medical schools (88%) reduced the scale and scope of curriculum operation. There were also some obstacles to having practical training in external institutions and meeting patients in person, but the training for clinical performance improvement using standardized patients or body models was relatively smooth. Fisher’s exact test results indicated no differences in the numbers of students, organization forms, region-specific online instructional methods, or operations of basic medical science practice and clinical clerkship training.
4. Student assessment under COVID-19 pandemic restrictions
Student assessments during COVID-19 are shown in Table 4. Among the schools, 20 (60.6%) conducted in-person mid-term or final exams, and 11 schools (33.3%) conducted a combination of in-person and online exams. Regarding clinical assessments, the most common response was in-person evaluations with 21 schools (63.6%), followed by report-based assessments (12.1%). The challenges associated with student assessments were mainly linked with securing exam venues and supervision due to social distancing measures for infection prevention (34.3%). Additionally, maintaining student safety and hygiene in exam venues (25.7%) posed difficulties. Seven schools (20%) reported challenges with online assessments during online classes. Regarding the introduction or continuation of online assessments post-COVID-19, more than half (53.1%) responded “no.” However, 49.4% showed positive responses or responses indicating ongoing discussions.
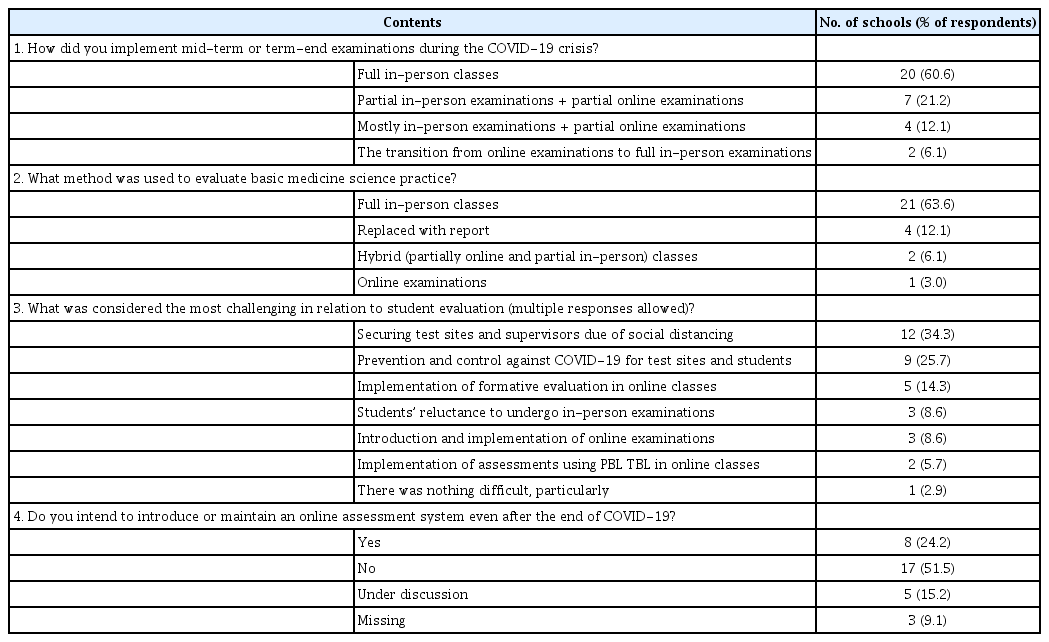
Student Assessments
5. Students’ assessment of their experiences with online learning
Table 5 shows student satisfaction by grade with lectures, discussions, experiments, and practice training. Students were highly satisfied with face-to-face online teaching for discussions, experiments, and practical training, but preferred VOD online for the lectures. One-way ANOVA to calculate differences in student satisfaction with the teaching methods between grades revealed significant differences for VOD, face-to-face, and blended learning lectures. For VOD, first- and second-year medical students, who mainly learn basic medicine and clinical medicine, were more satisfied than freshmen and prospective medical students (F=4.970, p<0.001). For face-to-face instruction, the first-grade premedical students reported higher satisfaction than that of first-, second-, and third-year medical students. In contrast, the third-year students who were completing their core clinical clerkship rotations had the lowest level of satisfaction with the face-to-face method, and there were also differences between the first- and second-year premedical students and the fourth-year medical students (F=8.271, p<0.001).

Student Satisfaction with COVID-19-Related Instructional Changes
DISCUSSION
We conducted this study in the form of a survey of medical school administrators and students to evaluate the overall effects of the COVID-19 pandemic on education at Korean medical schools; here, we discuss our results. First, there were no significant differences among the medical schools for location, school type, or entrance quota-specific countermeasures. Most schools had produced and distributed guidance on preventive measures against COVID-19 and on managing academic affairs when COVID-19 had initially emerged, immediately establishing personnel or organizations responsible for adjusting to changing demands. In addition, most schools had personnel dedicated to ensuring that online learning environments operated smoothly for students and professors. Globally, many medical schools and the Association for Medical Education in Europe presented guidelines on school management [13], production of learning materials [14], online class operations [15], practice [16], assessment [17], and leadership education [18].
Second, because the COVID-19 situation forced medical schools to shorten the duration of clinical clerkships or reduce the scope of the curricula, medical students demonstrated insufficient experience when they entered clinical practice. As noted earlier, in-person coursework that involved face-to-face interactions with patients faced some obstacles, although the practice courses using body models or standardized patients were implemented relatively smoothly. Medical school leaders took various measures to reinforce clinical clerkship programs. For example, Lee et al. [19] proposed role plays as an alternative practice method in to response to decreasing numbers of pediatric patients, increasing numbers of parents who refused to allow medical students to examine their children, and reduced numbers of ward rounds with three or more students.
Similar situations were faced by medical schools amid the COVID-19 pandemic across the world. The Association of American Medical Colleges recommended that US medical schools discontinue any student activities involving patient contact [20]. Thus, clinical clerkship training was replaced with remote medical treatment practice [4], virtual clerkships [5], or clinical simulations added to clerkships [6]. At this point, we want to stress the shortcomings of graduate medical education and clinical clerkships during the COVID-19 crisis. In this regard, providing students from the COVID-19 era with additional education programs as part of their medical internships is necessary. Additionally, we recommend future quantitative or in-depth qualitative cohort studies to measure the capabilities and professionalism of the doctors who were medical students during the COVID-19 pandemic era.
Third, leaders at most medical schools in Korea intended to keep providing online classes even after the end of the COVID-19 pandemic or were considering doing so. We predict that instead of operating regular classes online, as they did during the COVID-19 crisis, school administrators will utilize online learning environments for supplementary classes or remedial education to close learning gaps between students or offer advanced classes to academically talented students.
Samarasekera et al. found that during the COVID-19 crisis, medical schools had successfully introduced online learning using technology-oriented innovations [21], and we predict that the use of emergent technologies (e.g., artificial intelligence for adaptive learning, virtual simulation, and telehealth) for education will necessarily bring changes to post-COVID-19 medical education. Amid the spread of COVID-19, medical school leaders utilized a wide range of technologies to implement online learning, and scholars produced many reports on real-world applications of these technologies and teaching methods. For instance, McClure and William [22] in 2021 reported on the use of Gather, a metaverse platform, finding that it had been helpful for self-regulated learning.
Medical schools need to devise various teaching–learning strategies that could enable students to pay attention to online courses, given that many schools intend to utilize online classes in combination with in-person classes even after the end of COVID-19.
Fourth, many medical schools maintained in-person student assessments because of concerns about cheating on online student tests, although school leaders have used platforms such as Google Forms, Socritive (Showbie Inc., Edmonton, Canada), and Kahoot! (Clever Inc., Oslo, Norway) for formative assessments not related to academic records. To understand student responses to online testing, Yeo and Kim [23] analyzed students’ satisfaction with the online video tests conducted by graduate schools of medicine in Korea and found that students appreciated the easy access irrespective of location, the convenience, and the lack of travel time to test sites; however, they were concerned that unstable networks threatened their ability to complete their tests and expressed concerns about classmates’ cheating.
In fact, not only in Korea but around the world, school leaders expressed deep concerns about cheating during the COVID-19 pandemic [24]. However, schools in Korea used certain technologies to prevent cheating: keyboard authentication [25], PC cameras [26], face recognition [27], and motion detection [28]; nontechnical strategies to prevent cheating involved ethics statements for students and open-book exams [19]. In addition, there are reports where online assessments were conducted by Korean colleges related to health care [23]. Therefore, we conclude that fully online assessments can be conducted at medical schools and that medical school administrators expand online assessments in case of future disasters.
As a result of examining students’ satisfaction with online classes, they were satisfied with lectures in online classes as in other studies [29]; however, the discussions, experiments, and practice classes showed higher satisfaction with face-to-face classes. First-year premedical students preferred real-time face-to-face interactions with professors to VOD lectures. In contrast, the medical school students showed low overall satisfaction with all teaching methods except for VOD. First-year premedical students have described the first year of medical school as a critical transition during which they need to adapt simultaneously from being high-school students to being university and medical students [30]; we consider this the reason that these students need and benefit from more real-time interactions with their professors than students in other grades require. In contrast, first- and second-year medical students who are learning basic and clinical medicine seem to prefer repetitive individual learning through VOD.
The limitations of this study lie in the uneven grade-specific distribution of respondents, even though the link for the questionnaire was transmitted to medical students nationwide. There were many more first-year premedical students than students in any other grade. Nevertheless, this study is significant in that we received input from nearly all medical schools in Korea, our data referred to the initial stage of COVID-19, and we simultaneously targeted students and school leaders, the primary stakeholders in education.
In terms of future studies, we suggest that researchers conduct in-depth studies related to the study results stated above. We propose examinations of whether schools complied with their own COVID-19 guidelines. During the pandemic, medical schools promptly established emergency plans by referring to guidelines provided by various institutions in the areas of academic scheduling (classes and assessments), infection prevention, and clinical practice. Academic scheduling was based on the university’s guidance with input from KAMC, while individual medical schools created their own guidelines. Infection prevention followed guidelines from national agencies and hospitals, and clinical practice guidelines were set by hospitals, KAMC, and medical schools. Based on this experience, it was evident that effective decision-making involving multiple institutions is essential to successfully manage medical school operations during emergencies. This includes matters such as teaching and assessment methods, infection prevention, and clinical practice. To prepare for potential future pandemic scenarios, it will be necessary to identify decision-requiring matters, establish a hierarchy of decision-making for these issues, and develop “Emergency decision-making and academic operation measures” and relevant strategies.
We also propose, cohort studies of medical and graduate students who underwent training during the COVID-19 pandemic, studies on the effectiveness and long-term suitability of the variety of online COVID-19-era instruction and assessment methods for post-COVID-19 application, and studies on students’ emotional experiences during the COVID-19 crisis.
Acknowledgements
None.
Notes
Funding
This work was supported by Biomedical Research Institute grant, Kyungpook National Unviversity Hospital (2021).
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Author contributions
All authors contributed to set the concept and design of the research. SJN and SY contributed to data collection, analysis and interpretation. SJN and SY drafted the manuscript, reviewed, edited the manuscript. All authors read the manuscript critically, participated in revising the manuscript and approved the final manuscript.