Deeper look into feedback practice in an Indonesian context: exploration of factors in undergraduate clinical settings
Article information

Abstract
Purpose
The practice of feedback is influenced by the characteristics of students, teachers, and the clinical environment. Most studies on feedback have been conducted in Western settings with different sociocultural backgrounds to Indonesia. This study explores feedback in Indonesian clinical clerkship using a sociocultural lens and aims to provide an exemplar of adaptive practice relevant to non-Western settings.
Methods
This qualitative study was conducted using an interpretive phenomenology approach. Data were collected through focus groups with students and teachers and interviews with program coordinators. Data were transcribed verbatim and grouped according to data sources, coded, and analyzed thematically.
Results
Themes identified from the focus group discussions and interviews were categorized as student, teacher, and environmental factors. Student factors include dependence on feedback, tendencies to use a group approach, difficulties recognizing social rules, a perceived lack of resilience, and tendencies to doubt praise. Factors related to teachers include a high level of expertise, being extremely busy, having a strong commitment, and being unsure of students’ acceptance of feedback. Clinical environment factors influence interactions between teachers and learners and include high power distance and collectivistic values. A safe environment is needed to ensure effective feedback interactions.
Conclusion
High power distance, collectivism, and generational characteristics of students likely impact feedback practice in clinical settings. Designing a safe environment is essential for effective feedback practice.
Introduction
Current perspectives on feedback have been influenced by changing paradigms of medical education. Previously viewed simply as the process of teachers providing information to students on their performance; feedback concepts now acknowledge the complex interplay that occurs between teachers as feedback providers, students as feedback recipients, and the environment [1]. The Feedback Landscape Model describes how feedback interactions between teachers and students are influenced by many factors on both sides, as well as factors originating from the learning environment [2]. The process of feedback is not complete upon transmission of information to the student, it continues with the student interpreting the feedback and deciding whether to apply it to improve their performance. Current concepts of feedback place students in a central position of the process, where they are not merely recipients of information but active participants who respond to the message given and translate it into actions [3].
Several models have been developed to guide teachers in providing feedback [4-6]. However, challenges persist in the implementation of feedback practice, including in Asian countries such as Indonesia. Influenced by the high-power distance, Asian students perceive teachers as very knowledgeable and prefer feedback to be more directive [7,8]. The busy educational environment provides little time for feedback interactions. Feedback opportunities become more limited due to students’ reluctance to ask for fear of disturbing their teachers [7,9]. When feedback does occur, it is sometimes perceived as too vague; while praise (positive feedback) is viewed by students as less valuable because it often does not lead to improvement [9,10]. In Indonesia, a collectivistic society, feedback may sometimes be given in groups. Using this approach, the message tends to be general, presenting further challenges for students to apply information to their individual learning needs [11].
Many studies have shown that feedback plays essential role in clinical learning. As students are being exposed to clinical environment, they learn not just the knowledge and skills, but also the values and attitudes needed in the medical profession. Interactions with clinical teachers in the form of effective feedback help students process and make sense of their clinical experience in order to achieve competence and become the new member of the profession [12]. The different challenges identified in Asian countries have shown that sociocultural aspects play a major role in feedback practice. The hierarchical and collectivistic nature of Asian society affects the way feedback is sought, perceived, and processed [7,10,13]. Most literature on feedback is based on studies in Western settings with a different sociocultural background to Indonesia. Considering the importance of feedback in a dynamic clinical learning, and the characteristic challenges faced in the implementation of feedback practice in Indonesia, it is therefore necessary to explore further the factors affecting feedback practice in our setting. This study serves as the initial step to comprehending the interplay between factors and enriching the theoretical framework of feedback in non-Western sociocultural settings. This study aims to explore factors affecting feedback in clinical settings in Indonesia at the Faculty of Medicine Universitas Indonesia (FMUI). Through this study, we hope to discover how feedback interactions occur in clinical settings and how student, teacher, and environmental factors influence the practice of feedback. The results could serve as a starting point for developing a feedback model suitable for the hierarchical and collectivistic context found in Indonesian culture.
Methods
1. Study context
This study was conducted in clinical settings at FMUI. The curriculum consists of 7–8 pre-clinical semesters followed by four clinical semesters. The clinical phase includes a preparation module known as the Foundation of Clinical Practice (FCP), 1st and 2nd year clinical rotation modules, and a pre-internship module (MPI). The rotations involve various learning opportunities in classroom-based as well as clinical settings. The learning sessions, along with workplace-based assessments conducted throughout the rotations, provide extensive opportunities for feedback interactions. In order to become clinical teachers, teaching staff had to attend clinical teacher training which covers skills in teaching, including how to provide constructive feedback.
2. Design
This is a qualitative study using an interpretive phenomenology approach. Interpretive phenomenology was conducted by extracting meanings from the lived experiences of participants regarding the phenomena of feedback practice in their clinical settings with consideration given to how participants’ backgrounds might influence their perceptions [14].
3. Participants
Data was collected in focus group discussions (FGD) with students and clinical teachers, and interviews with academic program coordinators. We aimed for maximum variation sampling by ensuring representativeness in gender, academic performance, and clinical rotations in the student group; and representativeness in gender, teaching experience, and specialties in the clinical teacher group.
4. Data collection
Data were collected between December 2021 and February 2022. FGD and interviews were conducted using a virtual meeting platform. The first author (E.F.) acted as the moderator for all FGD and interviews, and a research assistant observed and took field notes throughout the process. The questions were developed following a review of the available literature, discussed with all the authors, and revised accordingly. Questions were set in order to explore (1) feedback practice in the clinical setting and (2) factors affecting feedback practice (the list of questions is shown in Fig. 1).
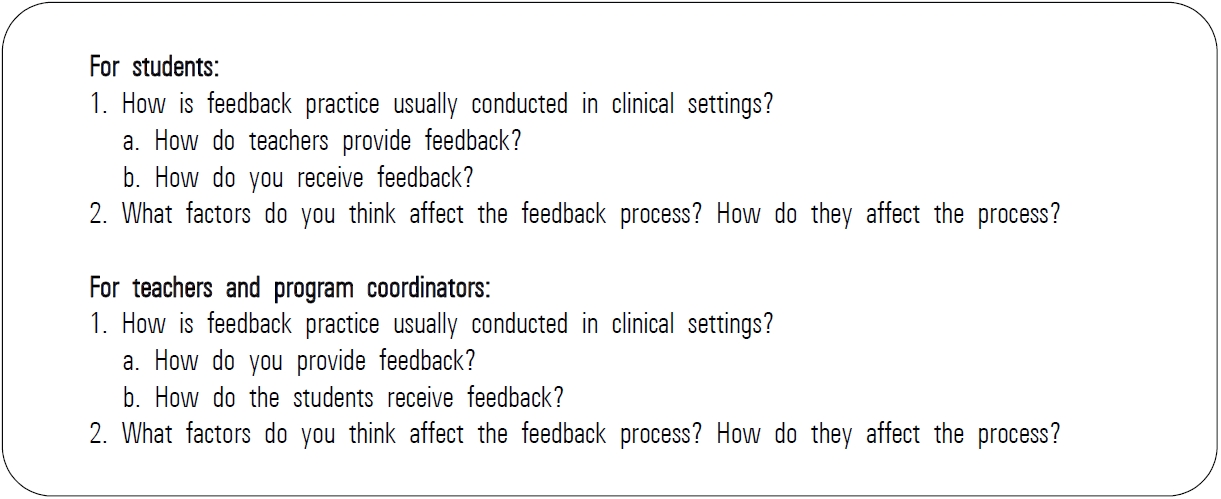
List of Interview and Focus Group Discussions Questions
5. Data analysis
Data were transcribed verbatim and grouped according to data sources, coded, and analyzed thematically. Independent thematic analysis was conducted by the first author using SCAT (Steps of Coding and Theorization) [15]. This method enables researchers to thoroughly analyze sentences from transcripts, identify important aspects, and paraphrase them. The next process was the identification of the concept and its arrangement into sub-themes and themes [15]. After initial thematic analysis, subsequent discussions were held by the research team for extraction and finalization of themes and sub-themes. Five of the authors (E.F., A.F., R.M., J.B., J.P.) are medical educators at FMUI and have an understanding of the clinical curriculum and its learning environment. The fifth author (L.R.M.R.) is a teaching faculty in the Faculty of Psychology, Universitas Indonesia with scholarly works on the generational impact on higher education. The seventh author (S.R.) is a clinician and an educational researcher from an institution in a different country with experience in qualitative research and prior work exploring sociocultural aspects of feedback. All of the authors are familiar with the concept being explored. Member checking was conducted by confirming the results with representatives of the students and teachers involved in FGD.
6. Ethical consideration
Ethical approval was given by the Research Ethics Committee Faculty of Medicine Universitas Indonesia with the approval letter number: KET-1114/UN2.F1/ETIK/PPM.00.02/2021. Participation in the study was voluntary, and informed consent was obtained from all participants. Data confidentiality was ensured through proper handling of data by the research team during the collection and analysis process.
Results
FGD for students were conducted in five groups: one group for students in the preparation module, three groups in 1st- and 2nd-year clinical rotations (ROT), and one group in the final semester. Each group consisted of 5–11 students with an age range of 22–24 years. FGD for teachers were conducted in several groups based on their teaching experience (senior [SNR] and junior [JUN] teacher groups), with each group comprising 3–9 teachers. Individual interviews were conducted with the program coordinators. The teachers involved in FGD and interviews had an age range of 38–67 years old. The characteristics of FGD participants and interviewees were shown in Table 1.
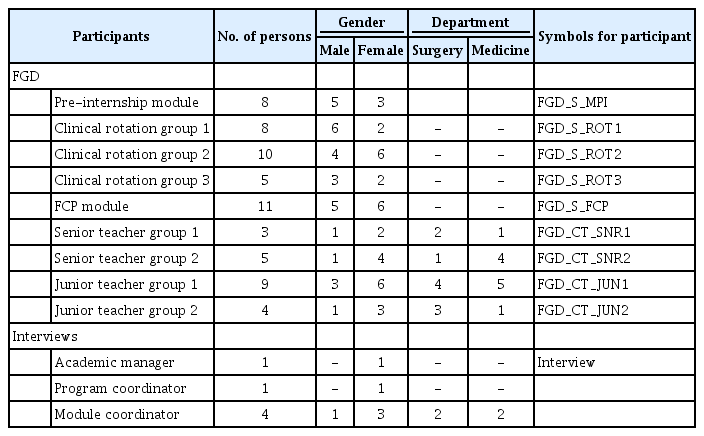
Characteristics of FGD Participants and Interviewees
The themes identified from FGD and interviews were described below along with representative quotes and depicted in Fig. 2. Factors affecting feedback practice were categorized as student factors, clinical teacher factors, and environmental factors.
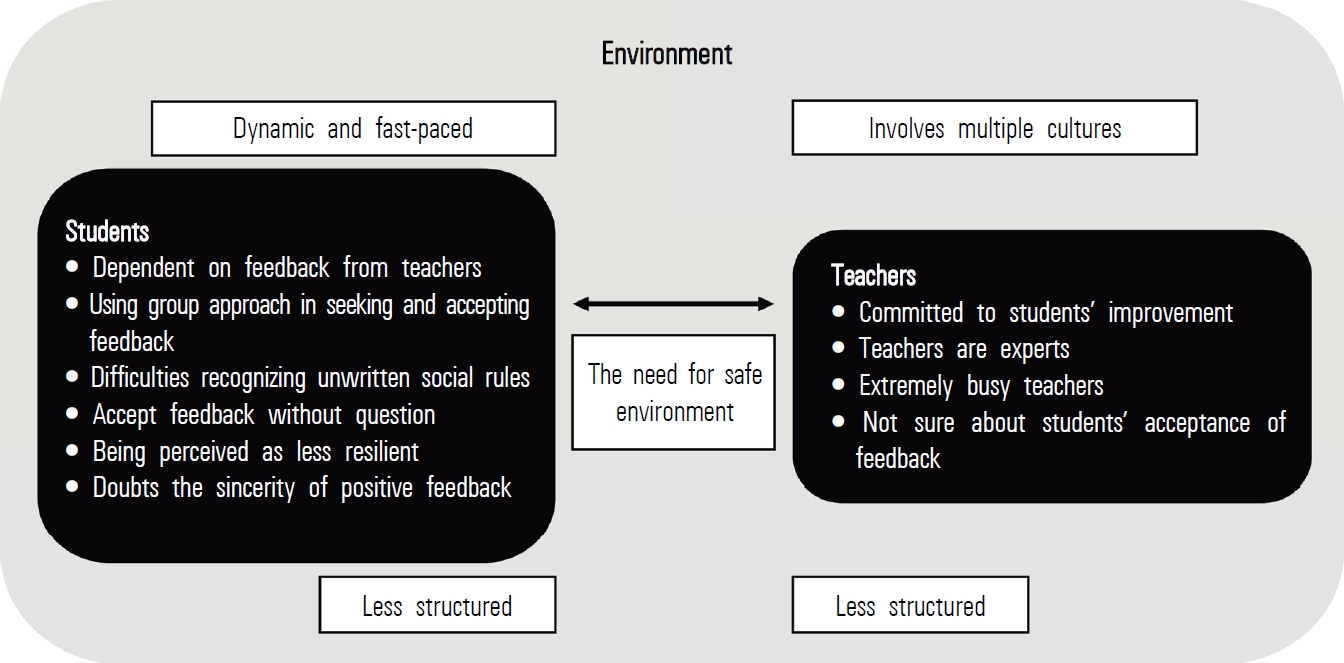
Student, Clinical Teacher, and Environmental Factors Affecting Feedback Practice
1. Student factors affecting feedback practice
Based on participant narratives, we were able to identify themes and map them into three categories: studentrelated, clinical teacher-related, and learning environment related. Below we provide a description of categories, themes, and representative quotes. We also indicated the source of the quotes; whether extracted from FGD or interview; and from student (S) or clinical teacher (CT).
1) Dependent on feedback from teachers
Students relied on feedback from teachers to determine whether their performance was satisfactory. Feedback served as means to provide insight and direction to reach the required standard. Feedback also highlighted important aspects of their performance, and sparked interest in the subject being taught.
“I feel enlightened, we are still learning, and we really need feedback. Without it, we are like blind people trying to find a way.” (FGD_S_ROT2)
2) Use of a group approach in seeking and accepting feedback
Students felt more comfortable completing activities, such as asking for feedback, in groups and discussed the feedback interaction they experienced with their peers.
“Not all students are eager to ask for feedback, but once we start answering one student, then the rest of them just cannot stop asking.” (Interview_02)
“The first thing I do after I receive feedback is tell my friends about it (laughed). We call it ‘passed-on’ knowledge, so we know ‘ok, when I deal with this doctor, I should do it this way’” (FGD_S_ROT1)
Feedback given in groups was acceptable for students on the condition that the message was not too personal. Some students enjoyed hearing feedback directed at their peers because they can learn without being put in the spotlight.
“The most enjoyable feedback is the one directed at someone else. That way I do not get the pressure of having to answer, but I still get the knowledge” (FGD_ S_FCP)
3) Difficulties recognizing unwritten social rules
Students experienced difficulties comprehending social norms and rules that apply in certain settings. This was challenging as not all teachers felt the need to explain clearly what they expect from the students and assumed that students should automatically understand these ground rules.
“Students are less sensitive today, even when we have set examples on how things should be done, that is not enough. We need to say, ‘please do this’.” (FGD_CT_ SNR1)
4) Accept feedback without question
Upon accepting feedback, students appeared as though they understand and agree with the message given. Students felt that they are in no position to question feedback and should follow instructions given by teachers.
“We’re still nothing, we’re not doctors yet, we need to be guided. And if the doctors teach us some questionable tips, while we are in their clinical setting, I do as instructed.” (FGD_S_MPI)
5) Being perceived as less resilient
Teachers found students to be less able to cope with problems, such as conflicting schedules in modules or accepting grades that are not yet perfect. A lower level of resilience was also observed upon dealing with feedback.
“I had a student that had to take some academic leave because she got scolded by the teacher. She said she has never been treated that way by her parents.” (FGD_CT_JUN1)
“When students were faced with conflicting schedules, they weren’t able to find a solution and just gave up.” (FGD_CT_JUN22)
6) Doubt the sincerity of praises
When students received praises, they were unsure of its sincerity. They feared that it might be sarcasm, instead of a compliment on their performance. This took place mostly when the feedback was not specific, or when no information was provided on aspects that require improvement.
“The doctors are way higher than us in the hierarchy. When they praise us, it just comes off as scary (laughed). When I answered correctly, the teacher said ‘Well, there you go. You do know, right? You’re smart.’ And I was confused ‘Is this positive feedback or sarcasm?’.” (FGD_S_MPI)
2. Clinical teacher factors
1) Committed to student improvement
The clinical teachers demonstrated commitment to their role. Despite modes of feedback delivery, students acknowledged that the teachers care for them, and the feedback was given to help improve students’ performance.
“I think our teachers care for us and are willing to adjust and expand their understanding to keep up with the current situation so that the students can meet today’s challenges.” (FGD_S_MPI)
2) Teachers are experts
Students perceived their teachers as very knowledgeable. They felt honored to be guided by such experts and were aware of the knowledge and experience gap that exists between them and their teachers. This condition made feedback from teachers very valuable.
“And we have doctors who actually wrote the clinical guidelines, so it’s a precious opportunity to learn from them, and effective feedback is the key to do that.” (FGD_S_ROT1)
Their position as experts were also perceived by teachers, which emphasizes the need for them to be able to provide knowledge and expertise when needed.
“The teachers should understand their topic well, they need to make sure that when their students ask a question they know the answer” (FGD_CT_SNR2)
3) Extremely busy teachers
Teachers had various responsibilities to attend to. In addition to providing healthcare services and teaching, some had organizational activities and were themselves pursuing academic study. This situation required them to prioritize, and multitasking became inevitable.
“And then it usually depends on the teacher’s situation. It could be that at that time the teacher’s schedule was so hectic, that could really affect the situation.” (FGD_S_ROT3)
4) Unsure of students’ acceptance of feedback
Teachers were not sure of students’ perceptions of the feedback they received. Students appeared to be receptive to it, but it still left teachers to wonder whether there were some elements of the feedback their students disagreed with.
“They seem to accept it, but I don’t know whether they feel like protesting inside.” (FGD_CT_SNR2)
3. Environment
1) Dynamic and fast-paced
The high number of patients demanding medical care made it necessary for healthcare teams to work efficiently. Their fast-paced way of working can sometimes be disrupted when students were involved in patient examinations.
“We have so many patients in our clinic. Faced with all that, of course we want to work fast, none of us wants to stay late. So, it is a bit difficult for students to be around in our clinic.” (FGD_CT_JUN2)
2) Involves multiple feedback cultures according to discipline
Each discipline had its own characteristics which affect the student-teacher interaction, including in feedback practice. Clinical teachers from surgical departments, for example, tended to be brief, while those in medical departments spent more time interacting with students.
“I find it very much affects feedback, teachers in the fast-paced emergency department tend to be direct, up to a point that they don’t use verbal padding.” (FGD_S_ROT1)
3) Less structured curriculum
Learning in clinical settings tended to be less structured compared to pre-clinical settings. There were no clear instructions for each activity, sessions re-scheduled due to changes in the clinics, and no explicit rules were provided to students on what is expected of their behavior.
“The module doesn’t provide instructions as to what we are expected to do, there is no guidance. So, it is up to our own initiative.” (FGD_S_ROT1)
4) Hierarchical
Hierarchical culture affected the way students perceive their teachers. Teachers were viewed as experts and therefore must be knowledgeable in recognizing the improvements needed in students’ performance. Students perceived feedback from teachers as far more accurate than their own reflections.
“I don’t think it’s necessary (to reflect), because the doctor would surely find more important aspects to improve. I like it better if the teachers just tell me what to improve because they know better.” (FGD_S_ROT1)
5) The need for a safe environment
A safe environment was deemed necessary by both students and teachers. It enabled students to become receptive to feedback. The environment was perceived as safe when teachers can show empathy, positioned themselves in a less superior manner, and were open-minded and willing to share their experiences with students.
“The environment should be safe, not hostile. If I meet a clinical teacher that often gets angry at students, I become scared and reluctant to interact, and tend to be defensive.” (FGD_S_MPI)
Discussion
Our study highlighted the ways in which sociocultural aspects affect feedback practice in clinical settings. Aligned with other studies conducted in Asian settings, it further confirmed the influence of cultural dimensions (high power distance and collectivism) on feedback, while also added the importance of generational characteristics to be considered in the way students approach feedback. The Feedback Landscape Model was used to discuss our findings and explain the interactions between each factor involved.
The identified student factors showed that students relied on feedback from teachers, had difficulties recognizing unwritten social rules and were often perceived by teachers as being less resilient. Upon receiving feedback, students can feel overwhelmed by negative emotions which prevented them from processing the message further. An ability to apply suitable coping mechanisms was crucial to derive the greatest benefit from the feedback provided [16]. The high-power distance between teachers and students further complicated the matter by causing hesitancy and fear to discuss or clarify the messages they receive [17,18]. This caused delays for teachers to recognize issues that occur with the acceptance of feedback. Students appeared to be receptive but could in fact be struggling to process feedback, and some might even experience distress [5]. Providing a safe environment and stimulating students with reflective questions during feedback interactions might assist students not only to receive feedback better, but also strengthen their resilience [16,19].
Students learned by observing peers, clinical teachers, and other healthcare professionals carry out their activities in addition to the positive reinforcement they receive [20]. Students needed to interact with their teachers due to their reliance on feedback and their need to learn social norms and values from the figures that they aspire to emulate. Generational differences between teachers and students might also influenced the interactions. Evidence suggested that for Generation Z, to which the present cohort of students belongs, human interactions along with the verbal and non-verbal cues contained within them can be challenging to comprehend, resulting in difficulties in recognizing unwritten social rules [21,22]. Students demonstrated collectivism in the way they approach this issue. Through sharing feedback experiences among themselves, students formed collective perceptions of their teachers and discover the correct ways to interact during feedback. However, this strategy may also be detrimental, as students may form preconceptions of teachers before they directly interact. The unpleasant experiences of their peers with some teachers can affect students’ perceptions and their behavior in any future interactions.
Teachers were perceived as knowledgeable figures from which students seek guidance and confirmation. This perception was also shared by teachers and strengthened their commitment to meet their students’ expectations. Teachers’ high level of expertise heightened the power distance and made feedback from teachers very valuable to students [10]. Teachers’ willingness to allocate time to engage in feedback interaction was perceived by students as an act of caring. Connections between teacher and student can be facilitated and strengthened through the practice of feedback.
The environment was characterized by the cultural dimension of high-power distance and collectivism. This power distance between teachers and students was evident in the way teachers were perceived as knowledgeable and competent figures, and the way students appeared to accept feedback (whether in the forms of corrective feedback or praise) despite not always being sure about the information given. It was also shown in the students’ preference for feedback to be directive instead of interactive. This was in alignment with findings from other studies in Indonesia, as well as Thailand (which has a similar sociocultural background); and somewhat in contrast to findings in the Western society [7,8,10,16]. The limited time available in clinical settings along with this condition created a rather brief feedback interaction, and the feedback message might not be accepted by students. This was similar to the findings of other studies concerning students’ acceptance of feedback [4,5], but in our study, the cultural dimension made the condition more prominent [11]. The practice of group feedback, another phenomenon not commonly found in Western society, often resulted in a vagueness to the message given, while the high-power distance created hesitancy to further clarify the message. Such a lack of clarification might hinder students from fully comprehending the quality of their performance. A safe environment became crucial for effective feedback interactions to occur. Within a safe environment, students can be open in conducting reflection, discussing their learning needs with the teacher, and agreeing the steps they need to take to improve their performance [5,17]. Teachers’ understanding of challenges faced by students in clinical settings helps students to feel accepted and builds a sense of belonging. Through effective dialogue, students’ psychological safety can be fostered as they build trust and the sense of being part of the community of practice in clinical settings [23].
This exploration of factors affecting feedback practice in FMUI elucidates how factors can interact with one another, characterizing the feedback process in Indonesian settings. The two cultural dimensions, high power distance and collectivism, along with the characteristics of Generation Z are found to play a prominent role in feedback practice. A safe environment has been identified as a requirement for enabling effective feedback interactions. The findings from this study can potentially serve as a foundation to construct a feedback model suitable for settings with similar sociocultural backgrounds.
The study was conducted in a single institution located in Indonesia’s capital city, and as such, the findings may not be entirely generalizable to other settings. However, considering current sociocultural values and attempts to analyze the results from the sociocultural lens, this study can be utilized as an example to explore feedback practice in different settings in order to support the quality of feedback.
Acknowledgements
None.
Notes
Funding
No financial support was received for this study.
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Author contributions
Conceptualization: EF, AF, RM, JB; methodology: JP, LRM; formal analysis: EF, AF, RM, LRM, SR; writing-original draft: EF; writing-review and editing: EF, AF, RM, SR; and approval of final manuscript: all authors.