Introduction
The World Health Organization (WHO) declared the novel coronavirus (COVID-19) first reported in December 2019 a global pandemic approximately 3 months after the outbreak [1]. However, this global pandemic has had a greater impact on countries that lack healthcare resources to deal with the disease and vulnerable groups with limited access to healthcare within those countries, thereby further intensifying health inequalities [2]. This was also observed in the COVID-19 vaccination rates, with only 32.6% of the populations in low-income countries vaccinated as of September 2023, which is lower than the global vaccination rate of 70.5% [3]. Furthermore, the impact of the emerging infectious disease is also reflected in the socioeconomic situation, with an expected 4.4% increase in income gaps between countries after COVID19, which had been decreasing before the pandemic [4]. Therefore, it is important to make efforts to address health inequalities through global cooperation because they are not limited to just one country and can affect not only healthcare but also society as a whole in all countries worldwide.
For global cooperation to resolve important global issues, the United Nations declared the Millennium Development Goals (MDGs) in 2000 and the Sustainable Development Goals (SDGs) in 2015, aiming to achieve them by 2030. MDGs are focused on having donor countries support the economic development of developing countries for poverty eradication based on the agenda discussed among donor countries in international development cooperation since the 1990s. However, SDGs are different in that they seek sustainable development through global governance to eradicate poverty and reduce inequality in all countries including developing countries [5]. This change in perspective can be examined in line with the fact that international health, which focused on supporting activities of developed countries to promote health in countries lacking resources since the foundation of the WHO in 1948, has led to the discussion on global health since the 2000s [6]. Global health differs from international health in that it pursues the health equity of all people within and among countries through international cooperation on all matters that directly or indirectly affect health beyond national borders [7]. This is in line with the SDG for good health and well-being, “Ensure healthy lives and promote well-being for all at all ages” [4]. Thus, it is necessary to focus on global health to understand and reduce health inequalities between and among countries for all people.
In medical education for training prospective doctors, discussions on determining global health competencies (GHC) that medical students must have for systematic global health education (GHE) have been ongoing. Guidelines about GHC for medical students were discussed by a consultative group, and the United States and Canada derived the core competencies of global health in a joint expert committee of the Global Health Education Consortium and the Association of Faculties of Medicine of Canada’s Resource Group on Global Health [8]. Moreover, in the United Kingdom, the Global Health Learning Outcomes Working Group presented GHC required for medical students as global health learning outcomes [9]. Recently, the Consortium of Universities for Global Health (CUGH) involving educational institutions and related partner organizations from numerous countries globally suggested Interprofessional Global Health Competencies (IGHC) that can be applied to GHE with a competency-based approach in various fields of study and classified GHC by level so that they can be applied to students of different levels [10]. IGHC of the CUGH were developed as a tool to measure the self-confidence of IGHC by Stuhlmiller and Tolchard [11], on which a validation study was also conducted.
Research on GHC in Korean medical education is in its initial stage and can be found in some studies. Kim et al. [12] surveyed the educational needs of students from health-related majors, including medical students, by applying IGHC of the CUGH to them. In addition, a Delphi study was recently conducted to identify GHC for Korean medical students based on GHC discussed overseas [13]. Despite insufficient discussion about GHC in Korean medical education, GHC are critical for nurturing future doctors to display leadership in global cooperation in the global community and lead changes in health inequalities from a macroscopic view. Accordingly, the 2022 Korean Doctor’s Role that defines the role and competencies of doctors also addresses public health in terms of social accountability and GHC in global health activities and healthcare policy engagement [14]. Furthermore, the accreditation in Korean medical education also recommends including content related to global health in the missions and graduation outcomes of medical school [15]. Therefore, the Korean medical education circle should also put efforts into training doctors with GHC and systematically prepare GHE based on GHC to put these efforts into practice.
However, although Korean medical schools highly perceive the need for GHE, there is a lack of systematicity in GHE because only a certain amount of time is allocated in the form of a class or special lecture within a specific program, rather than having an independent program [16]. Accordingly, GHE must be discussed based on GHC for Korean medical students, prior to which it is necessary to identify medical students’ perceptions toward GHC and analyze their educational needs. Thus, this study examined Korean medical students’ perceptions toward GHE and participation in global health activities and determined the priorities for educational needs based on the difference between the importance level and the current level of GHC.
Methods
1. Study design
This cross-sectional study aimed to investigate Korean medical students’ perceptions of global health and identify priorities for their educational needs.
2. Participants and data collection
The subjects of the study were medical school students in Korea who belonged to the Korean Medical Student Association (KMSA), and data were collected online for the entire month of December 2022 using Google Forms (Google LLC, Mountain View, USA). This study was approved by the Gil Medical Center Institutional Review Board of Gachon University (approval no., GBIRB2022-285). The notice for survey participant recruitment was posted by the KMSA, and the survey responses were collected automatically online. In total, 712 students participated in the survey, and 678 of them were selected for final analysis. Those excluded were 15 students who responded to the survey but did not agree to participate in the research and 19 students who belonged to the pre-medical course. There were 395 male (59.9%) and 264 female (40.1%) students, except for 19 respondents who did not reveal their gender. For medicine grade, 108 were in the 1st year (15.9%) 216 in the 2nd year (31.9%), 196 in the 3rd year (28.9%), and 158 in the 4th year (23.3%).
3. Instruments
The survey items to examine the current status and perceptions of Korean medical students of global health comprised the background of respondents, perceptions of GHE, and experiences and perceptions related to global health. The questionnaire was developed to meet the purpose of this study with reference to previous studies [17,18], and the items were revised considering feedback from experts. In the details of each item, the background of respondents included medicine grade and gender. For perceptions of GHE, there were multiple-choice questions on the adequacy of global health-related contents and experiences in the medical school curriculum, the need for GHE, and the curriculum type and appropriate phase for GHE. Regarding global health experiences, there were multiple-choice questions on whether the respondents have participated in global health activities, the types of activities they participated in, and the reasons for participation. For perceptions of global health, there were multiple-choice questions on interest in global health, interest in global health careers, and intention to participate in global health experiences abroad.
To identify priorities in educational needs based on GHC, we used GHC of Korean medical students from the study by Kim et al. [13]. GHC consists of 24 competencies in eight domains. For each competency, respondents were to rate on a 5-point scale their perceived importance level (1=not important at all, 5=very important) and the present level (1=very low, 5=very high).
4. Data analysis
For data analysis, frequency analysis was used to analyze the perceptions of GHE and the status of participation in global health activities. A chi-square test and an independent t-test were each used to test the differences in perceptions of global health and GHC depending on the respondents’ characteristics. Further, educational needs were analyzed by determining priorities through the difference between the importance level of GHC and the present level of students, for which the Borich needs assessment model and the Locus for Focus model were used [19]. The Borich needs assessment formula is as follows (RCL, required competency level; PCL, present competency level; R C L −
The responses collected from the survey were organized using Microsoft Office Excel 2016 (Microsoft Corp., Redmond, USA) and analyzed using IBM SPSS ver. 25.0 (IBM Corp., Armonk, USA).
Results
1. Perception of GHE and participation in global health activities
We investigated medical students’ perceptions of GHE and participation in global health activities. First, the key analysis results regarding perceptions of GHE are as follows (Table 1). Regarding whether global health-related content or experiences are properly carried out in the medical school curriculum, 245 (36.1%) out of a total of 678 respondents claimed that they “disagreed,” accounting for the highest ratio. Including 54 respondents (8%) who said they “strongly disagreed,” 44.1% (299/678) perceived that global health-related content or experiences were not properly carried out in the medical school curriculum. However, considering the need for GHE, 337 respondents (49.7%) “agreed” that GHE was necessary. Including 74 respondents (10.9%) who “strongly agreed,” 60.6% (411/687) perceived the need for GHE. As for the adequate type of curriculum for GHE, 457 (67.4%) chose “extracurricular program,” which is more than 217 (32%) who chose “regular curriculum.” In addition, the appropriate timing for GHE was classified by the characteristics of the Korean medical school curriculum into pre-medical that comes before the basic medical education, 1st and 2nd year of the pre-clinical course in medicine, and 3rd and 4th year of clinical clerkship course in medicine that is the basic medical education. The results showed that 327 respondents (48.2%) chose “pre-medical,” followed by 140 (20.6%) choosing “medicine” (3rd and 4th year), 101 (14.9%) choosing “medicine” (1st and 2nd year), and 99 (14.6%) choosing “continuous” (from pre-medical to medicine [1st–4th year]).
As for the participation of medical students in global health activities, 79 (11.7%) out of a total of 678 students responded that they had experienced participating in global health activities (Table 1). To determine the types and reasons for participation in global health activities, we analyzed the responses of 71 out of 79 students with experience participating in global health activities, excluding eight students who did not respond. For types of global health activities, 30 students (42.3%) chose “club activities related to global health,” whereas 24 (33.8%) chose “external programs related to global health” as the main types of activities they participated in. There were also global health activities such as “medical volunteer work or clerkship in university-organized overseas underdeveloped countries” and “cultural experience programs” in which approximately 5% of the students participated. Regarding the main reasons for participation, many students responded that they participated in global health activities because they were “interested in global health” (38/71, 53.5%) or they “considered necessary content for medical students” (20/71, 28.2%), whereas some claimed it was “for a career in global health” (8/71, 11.3%).
2. Differences in awareness of global health and GHC by characteristics
To analyze differences in perceptions of global health and GHC depending on respondent characteristics, we classified the groups by gender, grade, participation in global health activities, and participation in GHE and conducted a chi-square test. First, perceptions of global health were analyzed in terms of interest in global health, interest in global health careers, and intention to participate in global health experience abroad (Table 2). For interest in global health and interest in global health careers, all groups except a medicine grade showed a statistically significant difference at the significance level of p<0.05. By gender, there was a significantly higher ratio of female students who claimed to have interest in global health and its careers compared to male students. There was a significantly higher ratio of students who participated in global health activities and GHE who claimed to have an interest in global health and its careers. Considering the intention to participate in global health experience abroad, only gender and participation in global health activities showed a significant difference at the significance level of p<0.05. By gender, there was a significantly higher proportion of female students who claimed to have the intention to participate in the global health experience abroad compared to male students. In the group that participated in global health activities, there was a high proportion of students who claimed to have the intention to participate in the global health experience abroad.
Regarding GHC, we analyzed the differences in the perceived level of current GHC using an independent t-test. The results showed that there was no significant difference in gender and medicine grade at the significance level of p<0.05; however, there was a significant difference in participation in global health activities and GHE (Table 3). The perceived level of GHC was somewhat higher in female (mean±standard deviation [SD], 2.91 ±0.68) than male students (mean±SD, 2.87±0.66), and in 1st and 2nd year in medicine grade (mean±SD, 2.91±0.65) than 3rd and 4th year (mean±SD, 2.87±0.70), but there was no statistically significant difference. The perceived level of GHC was significantly higher in the group that participated in global health activities (mean ±SD, 3.20±0.72) than in the group that did not (mean±SD, 2.85±0.66), and it was also significantly higher in the group that received GHE (mean±SD, 2.92±0.67) than in the group that did not (mean±SD, 2.64±0.68).
3. Needs assessment for GHE
We analyzed the present and importance levels perceived by students for 24 items in a total of eight domains of GHC rated on a 5-point scale (Table 4). The total mean of the perceived present level of GHC was 2.89 (SD=0.68), whereas the total mean of the perceived importance level was 3.73 (SD=0.59), showing a difference of 0.84. The present level was highest in domain G (cultural diversity and health) with a mean of 3.33 (SD=0.87), and lowest in domain E (global health governance) with a mean of 2.44 (SD=0.87). The importance level was highest in domain C (determinants of health) and domain G (cultural diversity and health) with a mean of 3.97 (SD=0.75) and 3.97 (SD=0.79), whereas it was lowest in domain E (global health governance) at the present level with a mean of 3.30 (SD=0.82).
We used the Borich needs assessment model to analyze the educational needs based on the importance and present levels of GHC (Table 4). As a result of calculating the priorities according to Borich needs scores for each item, the item showing the highest priority was domain A (global burden of disease), item 2 “explain how to prevent based on the causes of major global epidemics.” However, the item showing the lowest priority was domain G (cultural diversity and health), item 2 “treat people from different backgrounds (racial, religious, social, cultural, gender) with respect and without any form of discrimination.” The domains including items with high priority were domain A (global burden of disease), domain B (globalization of health and healthcare), domain C (determinants of health), and domain D (healthcare in low-resource settings). In contrast, domain E (global health governance), domain F (health as a human rights), domain G (cultural diversity and health), and domain H (participation in global health activities) included items with relatively low priority.
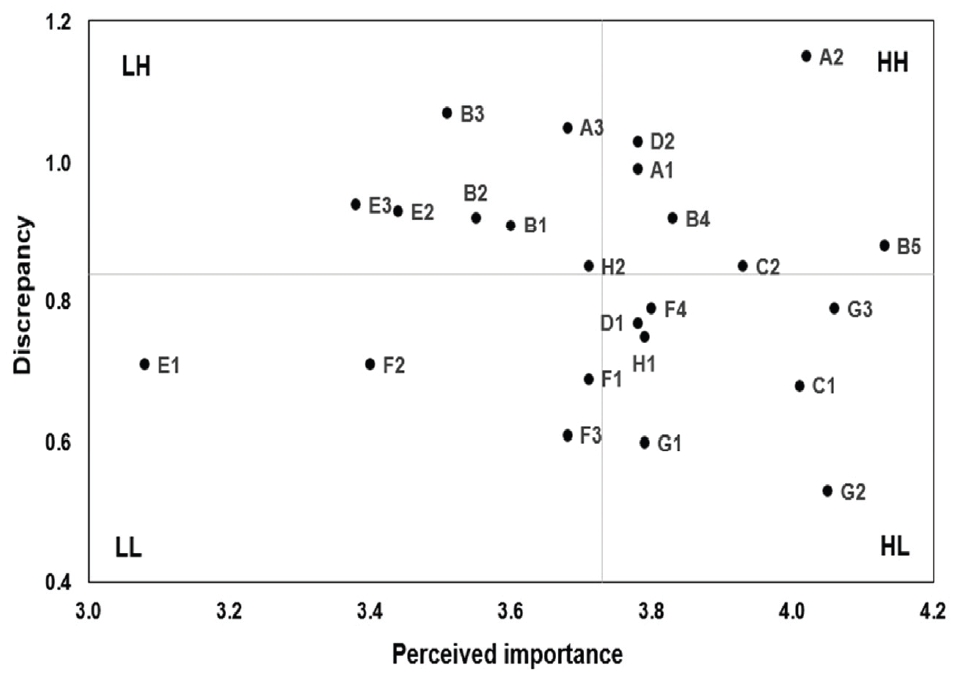
Moreover, in the Locus for Focus model, we analyzed the priorities of educational needs for GHC using a coordinate plane in which the horizontal axis represents the importance level, whereas the vertical axis represents the discrepancy between the importance and present levels (Fig. 1). According to the analysis results of the Locus for Focus model, the GHC located in the first quadrant, which shows a high importance level and high discrepancy between the importance and present levels, can be considered a top priority for educational needs. These are six items in total: items 1 and 2 in domain A (global burden of disease), items 4 and 5 in domain B (globalization of health and healthcare), item 2 in domain C (determinants of health), and item 2 in domain D (healthcare in low-resource settings).
Discussion
This study investigated medical students’ perceptions of GHE and participation in global health activities based on the results of a survey involving 678 medical students at medical schools in South Korea and analyzed the differences in perceptions of global health and GHC levels as well as the priorities in educational needs.
The results of analyzing perceptions of GHE are as follows. Although 12.1% (82/678) of the respondents perceived that GHE was sufficiently carried out in the Korean medical school curriculum, 60.6% (411/678) of the respondents perceived the need for GHE, showing a difference. This indicates that, in contrast to the highly perceived need for GHE among Korean medical students, insufficient GHE experience is provided within the current medical school curriculum. Kim et al. [16], who analyzed the status of GHE in Korean medical schools, confirmed a high percentage of schools assigning global health-related courses and special lectures in the form of 1- or 2-hour lectures in certain programs rather than having an independent program. Accordingly, this type of GHE is not perceived as a sufficient educational experience for students. Therefore, we can confirm the need to identify and discuss needs for GHE in Korean medical education because despite Korean medical students’ high perceptions of the need for GHE, the current medical school curriculum fails to sufficiently meet these demands.
As for the status of global health activities, 11.7% (79/678) of Korean medical students participated in global health activities, mostly club activities or external programs related to global health rather than activities organized by the medical school. Kim et al. [12] who studied health-related major students including medical students at a single university in South Korea also reported that 9.8% of the respondents participated in global health activities, showing a similar level. However, the actual participation rate in global health activities is low compared to the high perceptions of the need for GHE. Moreover, global health activities are mostly carried out by students at the individual level, as a higher percentage of students participated in club activities based on student autonomy or programs operated by external organizations rather than activities organized by the medical school. This may limit the opportunities to participate in global health activities. Considering that 53.5% (38/71) of the students who participated in global health activities responded that they were interested in global health, medical schools must make efforts to provide experiences or information about global health for students at the school level.
As a result of analyzing the differences according to the respondent characteristics in perceptions to global health, significant differences in global health and interest in its careers depending on gender, participation in global health activities, and participation in GHE, excluding medicine grade, were determined. There was a significant difference in the intention to participate in global health experiences abroad depending on gender and participation in global health activities. By gender, female students showed more interest in global health and its careers and had more intention to participate in global health experiences abroad. This result is consistent with Cox et al. [20] who analyzed students at a medical school and nursing school in the United Ststes and discovered that a higher ratio of female students with statistical significance showed an interest in global health careers than male students. Cox et al. [20] also confirmed that the female gender had a significant positive effect on interest in global health careers. Studies have explored gender differences in vocational interest, reporting that more women were interested in people-oriented fields and men in things-oriented fields [21]. In light of this, because global health activities require a multidisciplinary approach as well as communication and cooperation with people in various fields, women with an interest in people-oriented fields showed a significantly higher ratio of preference and intention to participate. Future research must conduct additional analysis to specifically reveal gender differences in interest in global health among Korean medical students.
Furthermore, those who participated in global health activities and GHE showed a high interest in global health and its careers. A study analyzing the factors affecting the interest in global health careers revealed the relationship with global health experiences and confirmed a significant positive relationship in research activities among global health experiences [20]. This implies that global health activities or educational experiences of Korean medical students may also be related to interest in global health. Accordingly, future research must analyze the effect of Korean medical students’ global health activities or educational experiences on interest in global health and classify global health activities into specific types. Moreover, those who participated in global health activities and GHE showed high intention to participate in global health experience abroad, but only those who participated in global health activities showed a statistically significant difference. As 93.1% of the courses in global health curriculums were lectures in current GHE in Korean medical schools [16], many students might have experienced GHE through lectures. On the contrary, as global health activities involve student participation through club activities, external programs, medical volunteer work, and clinical training, there may be a difference in the method of experience from GHE. Moreover, as intention is a key factor in predicting actual behavior [22], it is necessary to understand the intention to participate in global health as it can predict future participation in global health activities. As the significant difference in the intention to participate in global health is not found in participation in GHE, we can consider that GHE in the form of lectures may have limitations in attracting participation in global health activities. This implies the need to provide educational experiences in various teaching methods including student activities other than lectures in GHE.
As a result of analyzing the differences according to the respondent characteristics in the level of perceptions of GHC, there was no significant difference according to gender and medicine grade, and the level of perceptions was significantly higher in those who participated in global health activities and GHE. These results are consistent with the survey on perceptions of IGHC conducted on students from health-related majors including medical students in South Korea, where the level of perceptions was significantly higher in those who participated in global health activities [12]. This is also in line with a study on nursing students in South Korea where the level of perceptions was significantly low in those who did not have experience participating in GHE [17]. Moreover, Lanys et al. [23] surveyed students who participated in the 10-year global health elective course at a medical school in Canada and examined their perceptions of the effect of the global health course on the improvement of GHC. The ratio of students perceiving that there was an effect on improving GHC remained high even after graduation. In addition, study results on nursing students in South Korea revealed the effect of GHE programs on improving GHC [24,25]. This implies that GHE or global health activities of medical students can be related to improving the level of perceptions of GHC. This raises the need to conduct research to determine the effect of GHE or health activities on GHC of Korean medical students.
The results of analyzing GHC educational needs showed a statistically significant difference between the present and importance levels in all 24 items of eight domains comprising GHC. In total, eight items were determined for the priorities in educational needs, with four items in first priority and four in second priority. These items belonged to the global burden of disease, globalization of health and healthcare, determinants of health, and healthcare in low-resource settings among the domains of GHC. This result is consistent with the analysis of educational needs of health students including medical students in South Korea that confirmed top priority items in the global burden of disease and globalization of health and healthcare [12]. We examined the course topics related to GHC found in the study by Kim et al. [16] who analyzed the current status of GHE in Korean medical schools and discovered that approximately 90% of schools covered content related to global health governance, and most schools included this as a course topic. However, only approximately 50% of the schools in this study covered content related to the global burden of disease, globalization of health and healthcare, and determinants of health that are top priority educational needs in GHC as a course topic. The percentage for healthcare in lowresource settings was even lower at approximately 30%. Global health governance may have been derived as a domain that does not have high priority in educational needs since a high ratio of schools covers this as a course topic. However, considering that it is the lowest domain in terms of the perception level of GHC, it is necessary to identify specific contents through further research. Although the global burden of disease, globalization of health and healthcare, determinants of health, and healthcare in low-resource settings are domains with the first and second priorities in educational needs, not a high ratio of schools has included them as a course topic, which raises the need to improve course topics in current GHE.
Moreover, the global burden of disease, globalization of health and healthcare, and healthcare in low-resource settings showed lower levels of perception than the overall average of GHC, which is consistent with the studies on Korean nursing students [17,26] and US graduate students [11] in which the global burden of disease and globalization of health and healthcare were low in terms of perceptions of GHC. This showed consistent results with previous studies in terms of Korean medical students’ perceptions of GHC. Because the priorities for educational needs in these domains are high, efforts must be made to improve GHE so that GHC can also be enhanced in light of the priorities.
In conclusion, global health is important in medical education for nurturing future medical professionals who understand health inequalities from a macroscopic perspective and participate in various activities to solve them. However, although perceptions of the need for GHE are high in Korean medical education, discussions on GHE are still at an early stage, and research deriving the GHC of medical students has been conducted only recently. This study has significance in making the first attempt to identify the level of perceptions of GHC and determine priorities in educational needs for GHC among medical students in South Korea, which will lay the groundwork for developing systematic GHC-based curriculums. Furthermore, the differences found in the level of perceptions of global health and GHC depending on participation in global health activities and GHE indicate that the role of medical schools is necessary for global health activities and education to improve GHC.